


To Issue 186
Citation: Pidding M, “Deliverability, Acceptability, Availability: Assessing the Evolving Strengths of Microneedle-Based Drug Delivery”, ONdrugDelivery, Issue 186 (May 2026), pp 96–100.
Dr May Pidding explores the growth and future potential of microneedle technology and its suitability for a broad range of drug delivery applications, specifically presenting the case for the accelerated uptake and wider adoption of Microneedle Array Patch (MAP) technology.
There is a paradox at the heart of medical science. Viewed from one angle, it is a world rooted in evidenced ideas; viewed from another, it is driven by a belief that truths are not absolute and that knowledge is, at best, provisional.
This acceptance of uncertainty acknowledges the vast complexity of human biology, an evolving understanding of optimal medical approaches and the difficulties associated with discovering, developing and delivering therapies that make a difference to patients. Perfect solutions are rare. More often, variables must be accommodated and compromises accepted in the interests of outcomes. An example of this is covid-19 vaccines, which, although developed at incredible speed, demanded an unprecedented investment of resources.
When it comes to more traditional, default methods of drug delivery, unavoidable compromises are widely evident, whether it is the requirement for medicines to be distributed and stored in cold chain conditions, the need for patients to travel to healthcare facilities for supervised administration, or for undesirable delivery forms to be accommodated by those with either needle phobias or problems swallowing. However, innovative alternatives are now available that address legacy delivery shortcomings and offer additional new benefits.
An example of this is microneedle technology, specifically microneedle array patch (MAP) technology, which is now proven and available for customised projects in the form of the proprietary AccuTip MAP platform from LTS (Figure 1).
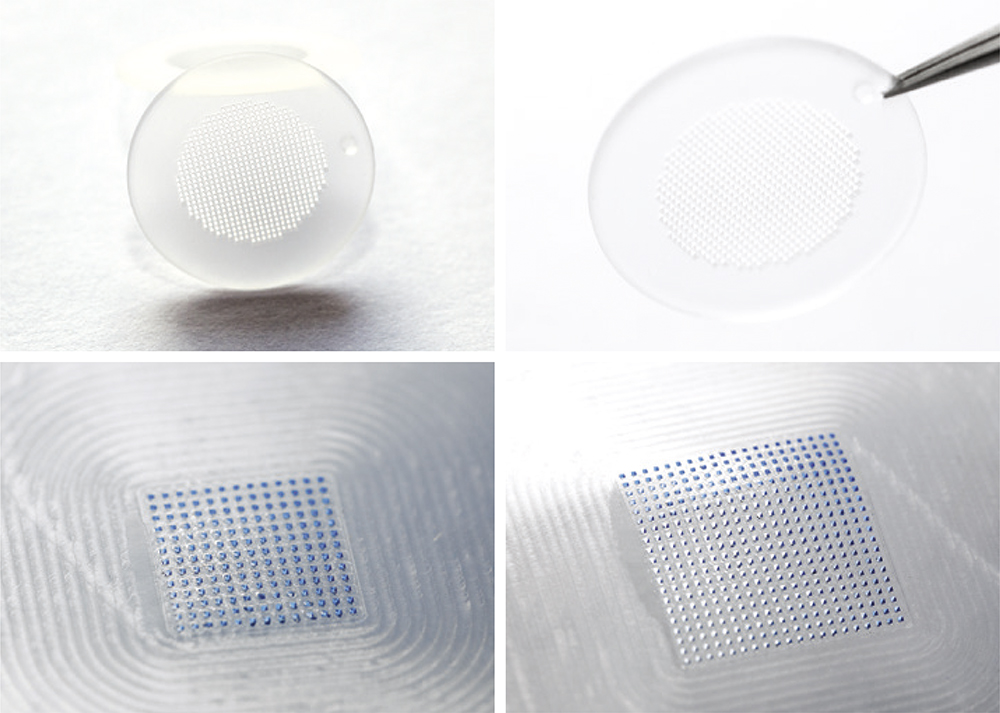
Figure 1: Different microneedle array patch designs.
MAPs leverage the skin’s unique properties, enabling minimally invasive, pain-free drug delivery with the potential to enhance therapeutic outcomes and improve patient comfort and compliance, while fundamentally changing how and where patients can access treatments and vaccines. This transformative technology has displayed effectiveness in proof-of-concept trials, as well as suitability for a wide variety of molecules including biologics, vaccines and small molecules. The flexibility and configurability of MAPs may allow them to overcome the limitations of legacy injection systems.
THE SKIN: A GATEWAY TO SYSTEMIC DELIVERY
While the skin is easily accessible and immunologically active, to date it has been underutilised as a route for systemic drug delivery. Largely, this has been because drug delivery options have been limited to the delivery of small molecules at relatively low doses.
However, scientific advances in intradermal therapeutic systems, such as MAP technology, can overcome these limitations. Microneedle patches, typically consisting of arrays of hundreds of microscopic needles per patch, can painlessly penetrate the outer layers of the skin and deliver APIs directly to the viable epidermis or dermis. Here, substantial immune cell populations, capillary networks and microvascular structures enable efficient uptake while avoiding deeper tissue penetration and the pain associated with intramuscular or subcutaneous injections. Additionally, because the route of delivery bypasses the gastrointestinal tract and liver, MAPs avoid the reduction of drug efficacy caused by the first-pass effect.
“MAPs ARE NOT A SINGULAR DESIGN CONCEPT BUT A VERSATILE PLATFORM.”
Crucially, MAPs are not a singular design concept but a versatile platform. Modern systems typically use dissolvable polymer microneedles that encapsulate the API within the needle tips themselves. Upon application, the needles dissolve in the skin, delivering the drug in alignment with the dosing protocol. Their versatility is underlined by the fact that the rate of release of a particular molecule can be controlled through formulation with either slow or quick-release polymers, depending on the target profile of the drug product.
From a patient perspective, the experience is simple and largely pain free. In terms of healthcare infrastructure and investment, it removes many of the restrictions associated with traditional delivery methods, avoiding the involvement of trained healthcare professionals (HCPs), eradicating injections and, in many cases, curtailing the need for deep-freeze cold chain logistics.
FROM CONCEPT TO CLINIC
Microneedle technology has been in existence since the 1970s but, for many years, it has remained largely confined to academic research. Manufacturing complexity, dosing precision and scalability have posed significant challenges, and the absence of a clear regulatory and commercial pathway reinforced the perception of MAPs as an emerging, perhaps even speculative, technology.
However, today, the picture is very different (Figure 2). Significant advances in materials science, precision manufacturing and process automation in recent years have transformed MAPs into a credible, clinically validated delivery platform.1 A total of 128 registered clinical trials using microneedle technology for therapeutic and diagnostic purposes have been registered globally, covering applications ranging from vaccines and biologics to high potency small molecules.2
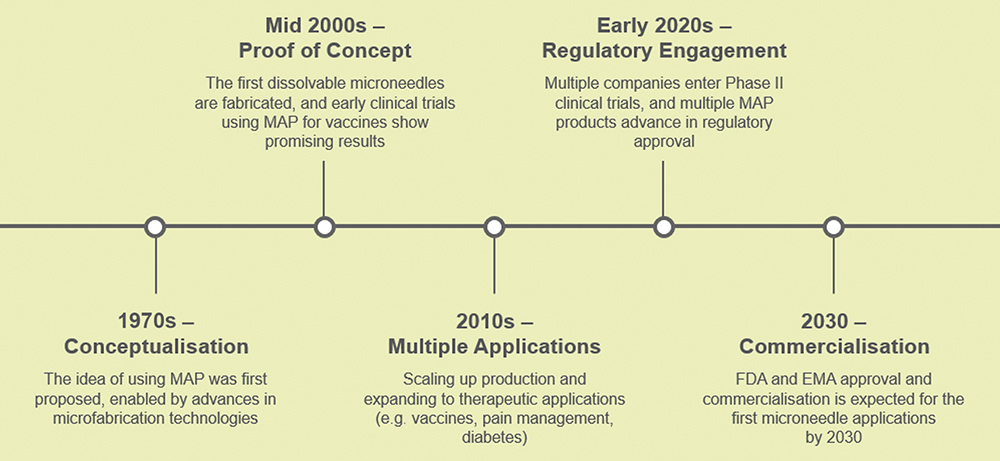
Figure 2: The evolution of microneedle-based drug delivery.
These trials support a growing body of evidence that demonstrates the capabilities of MAPs in achieving comparable results to established delivery routes in terms of efficacy, safety and dose consistency, with many studies evidencing improved tolerability among patients.3
“THE ABILITY OF MAPs TO MAINTAIN OR IMPROVE EFFICACY OF VACCINES IN A PATIENT-FRIENDLY FORM HAS DIRECT AND SIGNIFICANT ADVANTAGES FOR LARGE-SCALE PROGRAMMES – SUCH AS GLOBAL VACCINATION INITIATIVES – IN TERMS OF LOWER COST, GREATER SUPPLY RESILIENCE AND WIDER REACH.”
One such example is a Phase I investigator-initiated clinical booster study conducted by LTS on a licensed hepatitis B vaccine, which compares delivery via MAP with the traditional intramuscular injection (Figure 3). The results showed that MAP delivery generated a stronger immune response, both with and without the use of an applicator. Notably, unlike the licensed vaccine, this enhanced response was achieved without adjuvants and using a delivery method that is inherently pain free. As such, the ability of MAPs to maintain or improve efficacy of vaccines in a patient-friendly form has direct and significant advantages for large-scale programmes – such as global vaccination initiatives – in terms of lower cost, greater supply resilience and wider reach.
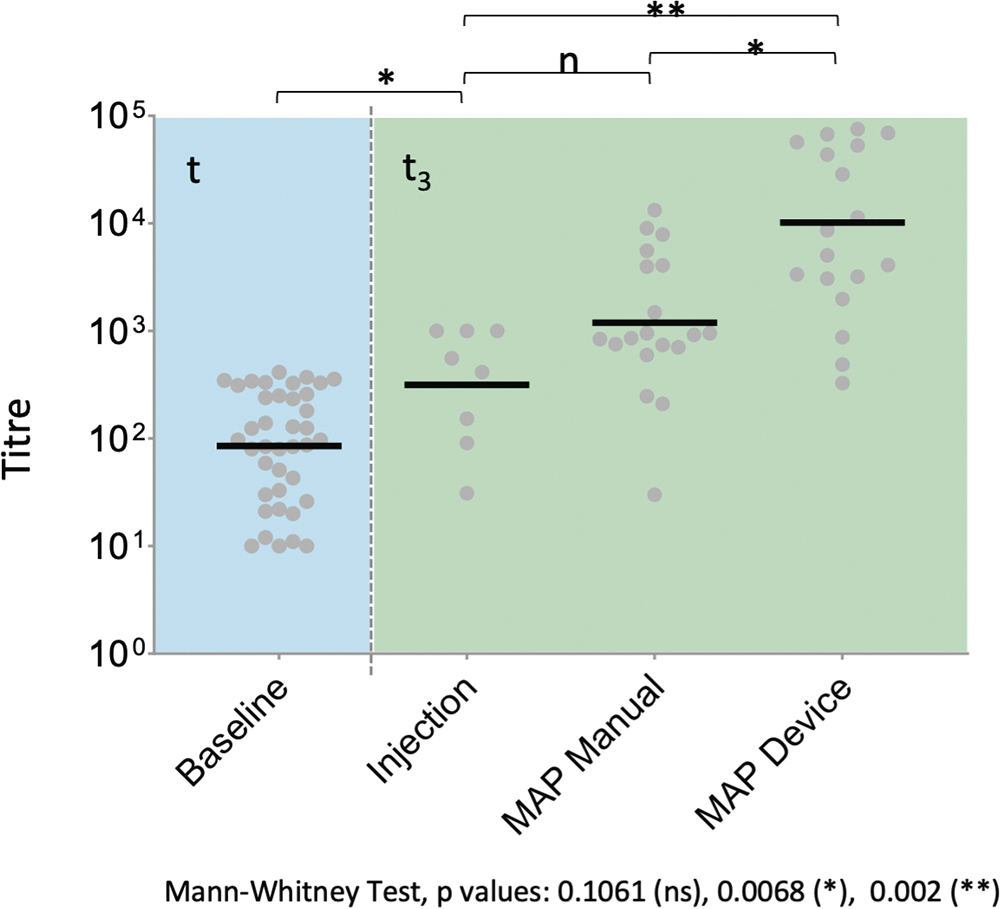
Figure 3: Phase I investigator-initiated clinical booster study.
MITIGATING COMPROMISE: MAPs VERSUS CONVENTIONAL DELIVERY ROUTES
Every drug delivery system incorporates a degree of compromise, leading to crucial questions regarding the level and nature of the trade-offs required and whether they can be accepted. Oral delivery is convenient but unsuitable for most biologics and vaccines, and problematic for patients with difficulty swallowing. Injections offer broad applicability but bring pain, anxiety, the need for trained administrators or patients proficient with self-administration and the risk of needlestick injury and infection, all of which can converge to impair adherence and compliance. In many cases, clinical resources might also be required to support drug delivery, placing a burden on healthcare providers and inconveniencing patients, with the impact felt disproportionately by those with limited mobility or access to care. For the healthcare payers, such burdens can be associated with considerable financial cost.
MAPs resolve some of these key points of friction. By enabling simple, self-administered, pain-free delivery, they remove many of the practical and psychological barriers that prevent patients from fully engaging with and adhering to their treatment regimens. For individuals with needle phobia, children and the elderly, this represents a transformative shift – particularly in the context of managing chronic conditions at home. Indeed, LTS’s recent study on multiple sclerosis treatment demonstrates that MAP technology has great potential to provide an alternative to injectable therapy systems.4
From a wider healthcare ecosystem perspective, MAPs can reduce reliance on HCP time, lower the burden on clinical facilities and support decentralised care models. These benefits extend beyond convenience for individuals; they contribute to more resilient, inclusive and affordable healthcare systems that work better for patients of all ages and physical capabilities.
Application by MAPs enables patients to maintain their regular lifestyles, ensuring that daily life is not dictated by their disease or treatment regimen. In addition, better adherence due to ease of application leads to significant reductions in hospitalisation rates due to non-compliance to treatment.
One Platform, Many Possibilities
One of the most compelling attributes of MAP technology is its flexibility. The same underlying platform can be adapted to deliver a wide range of molecules, including vaccines, biologics, mRNA formulations and small molecules. The needle geometry, matrix composition, dose loading and release kinetics can all be tailored to the specific requirements of a given API and indication. This configurability supports applications ranging from mass vaccination to more targeted treatments, where smaller batch sizes and precise dosing can be accommodated in a GMP-compliant and economically viable way. As such, patients are not forced to adapt to delivery systems that are optimised for scale but, rather, can receive medicine via convenient delivery systems that are suited to their specific treatment regimens and personalised medicine needs.
There are few barriers to equitable drug access as pervasive as cold chain requirements. For many biologics and vaccines, maintaining stability from manufacture to administration can demand ultra-low temperature storage. In regions with limited infrastructure, or in emergency response scenarios, this requirement alone can determine whether a therapy can be made available at all. MAP technology has demonstrated real potential in addressing this challenge.
In a study conducted by LTS using a lipid nanoparticle (LNP) formulated mRNA rabies vaccine, doses delivered with MAPs achieved protective antibody titres comparable with intramuscular injection (Figure 4). Importantly, these results were obtained with storage conditions of 2–8°C for the MAPs – far less demanding than those associated with the original bulk material, which was stored at -80°C.5
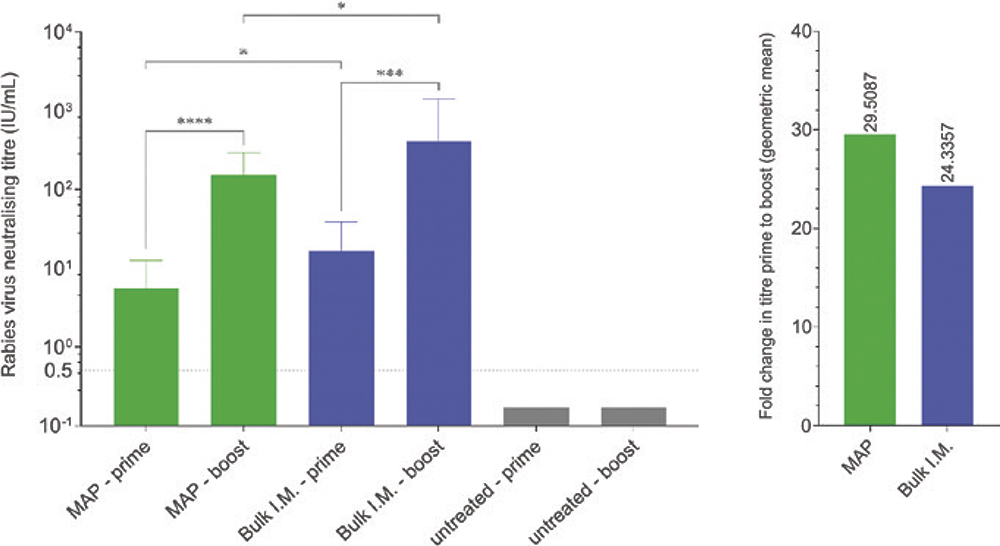
Figure 4: mRNA-LNP rabies vaccine preclinical trial in guinea pigs.
“MAPs COULD SIGNIFICANTLY REDUCE – OR EVEN ELIMINATE – COLD CHAIN DEPENDENCY FOR CERTAIN THERAPIES. IN DOING SO, THEY DIRECTLY ADDRESS ONE OF THE MOST PERSISTENT STRUCTURAL INEQUALITIES IN GLOBAL DRUG DELIVERY.”
Taken together, these findings suggest that MAPs could significantly reduce – or even eliminate – cold chain dependency for certain therapies. In doing so, they directly address one of the most persistent structural inequalities in global drug delivery.
MANUFACTURING, REGULATION AND THE MYTH OF “EARLY ADOPTER RISK”
While the positive momentum around MAPs as an innovative drug delivery method has continued to build over time, adoption has been hindered to a certain extent by hesitancy surrounding manufacturing complexity, regulatory uncertainty and the comparative costs of individual products. It should be acknowledged that these concerns were not without foundation in the earlier stages of MAP development. However, they have subsided as the technology has evolved and matured.
Through a combination of process optimisation, automation and modular manufacturing design, MAP production can now be scaled in a controlled, cost-effective manner. Modern approaches focus on optimising small-scale processes and then replicating them through modular expansion. This strategy reduces upfront capital investment while preserving flexibility and regulatory control, providing a managed pathway for a technology that is readily available for development and clinical studies.
Regulatory engagement has evolved in parallel. As a manufacturing authorisation holder in Germany, LTS operates in continuous dialogue with healthcare authorities, clarifying any perceived points of uncertainty while ensuring that MAP development aligns with expectations around dosing consistency, materials compliance and patient safety. This proactive approach de-risks clinical progression and shortens time to market for pharmaceutical partners.
MATCHING DRUG DELIVERABILITY AND PATIENT ACCESSIBILITY TO COMMERCIAL AVAILABILITY
Equality in accessibility does not mean offering everyone the same solution. It means ensuring that everyone can access treatment in a way that works for them physically, psychologically and practically. MAP technology represents a meaningful step towards that goal. By removing needle-related pain, reducing cold chain dependence, enabling self-administration and supporting a broad range of APIs, MAPs challenge long-accepted norms in drug delivery and expand the options available.
The conclusion is clear: access to life-enhancing medicines will only become more equitable by designing drug delivery solutions that adapt to patients, wherever they are and whatever their circumstances. Having long progressed beyond experimental early stages, MAPs are now proven as a market-ready technology that offers first-mover advantage to forwards-thinking organisations focused on overcoming the challenges associated with legacy delivery routes. Through a combination of API deliverability, patient acceptability and clinical availability, MAPs today are helping establish tomorrow’s new era of patient centric medicine.
REFERENCES
- Choo JJY et al, “Microarray patches: scratching the surface of vaccine delivery”. Expert Review of Vaccines, 2023, Vol 22(1), pp 937–955.
- Moawad F, Pouliot R, Brambilla D, “Dissolving microneedles in transdermal drug delivery: A critical analysis of limitations and translation challenges”. J Controlled Release, 2025, Vol 383, art 113794.
- Arya J et al, “Tolerability, usability and acceptability of dissolving microneedle patch administration in human subjects”. Biomaterials, 2017, Vol 128, pp 1–7.
- Brodkorb D, Scherr S, Schlüter S, “A promising alliance in multiple sclerosis treatment. Microarray patch for the administration of beta interferon: A preclinical minipig study”. J Drug Del Sci Tech, 2025, Vol 114, art 107460.
- “LTS receives grant of $1.2 Million to support the development of thermostable mRNA formulations for Microneedle Array Patches”. Press Release, LTS, Dec 6, 2023.