

Ciation: Redding BK, “Designing an Ultrasound-Enabled Patch for Insulin”. ONdrugDelivery Magazine, Issue 49 (May 2014), pp 22-26.
Bruce K Redding Jr tells the story of the design and development of the U-Strip™ Insulin Transdermal Delivery System.
ELECTRONICALLY ASSISTED TRANSDERMAL DEVICES
There are several approaches used to assist transdermal delivery electronically, including iontophoresis, laser and sonophoresis ultrasound. These systems are designed either to increase the flow of drugs across the stratum corneum or to microporate the skin, to allow the delivery of macromolecules across the stratum corneum into the dermis or underlying tissue.
Such electronically assisted transdermal delivery devices (TDDs) often use an outside electronic system, which is not connected to a drug-containing patch, or the patch has electrodes within it to assist in ionic transfer. Direct connection to a disposable transdermal patch is often impractical because the electrodes, or ultrasonic transducer system, are not disposable.
Any electronic signal sent through the TDD to liberate insulin from the patch must be reviewed for damage to the drug itself. Iontophoresis was found to induce electrical charges to the insulin which was found to be deleterious to its protein structure. Laser and infra-red transmissions through the TDD photo-damaged the insulin.
Sonophoresis, the application of sinusoidal ultrasound through the skin, can induce cavitation, which can usefully microporate and develop micro pathways through the skin, but the explosive energy of cavitation can heat and damage the insulin, and cause severe damage and discoloration to the skin. Therefore a two-step approach was tried – initial microporation of the skin, after which a patch containing insulin was placed over the skin site. Problems with this approach included insufficient intra-application dose control as the absorption of the porated skin section can have an irregular penetration diameter through the skin; and that the skin tends to seal such capillary punctures on its own.
So we faced the following challenges for transdermal insulin delivery:
- Insulin is too large a molecule to pass passively through the skin.
- Skin enhancing chemicals could interact with insulin and denature the drug.
- Ionotphoresis could denature the drug.
- Laser or IR transmissions sent through the skin would photo-damage the insulin.
- Sonophoresis, sinusoidal ultrasound, through cavitation can cause severe damage to the skin and discolouration and lead to a breakdown of the drug.
We decided to go for ultrasound. Of all the electronic systems, ultrasound offers the most promising capability for transdermal insulin delivery. It has an ability “push” the drug from the TDD through the skin because of vibrational energy. We were aware that sinusoidal ultrasound-induced cavitation could damage both the drug and the skin. Therefore, in order to use ultrasound, the problem of cavitation had to be defeated.
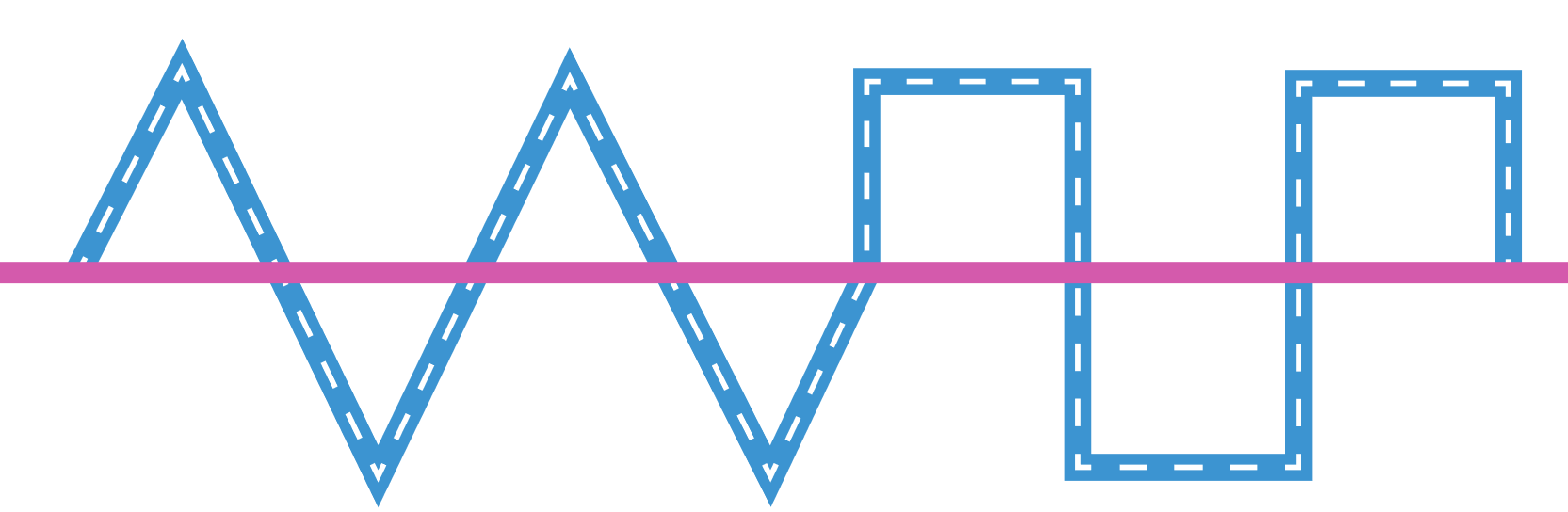
At this point in our design attempt to bring an insulin TDD into fruition, the first obstacle was to find a method to deliver a 6,000 Da compound through the skin. That was accomplished by the use of the sawtooth ultrasonic transmission, and through the skin pathway choice of targeting the skin pores for dilation. Our next problem was cavitation via traditional ultrasound. This was solved by interrupting one waveform with a switch to another wave form. In this case sawtooth to square wave (see Figure 1).

Figure 1: Alternating the waveform of the ultrasonic transmission eliminated or reduced the effect of cavitation.
ALTERNATING ULTRASONIC WAVEFORM DYNAMIC
A unique alternating ultrasonic transmission was developed whereby ultrasound wave forms are altered just before cavitation could develop. An unusual function of sawtooth waves is the ability, when contacting a surface, to transverse that surface laterally instead of vertically. So a sawtooth wave transmission can flex the pores of the skin, dilating the skin pathway into a larger diameter. The sawtooth wave has been shown to dilate and enlarge human skin pores from the normal diameter of approximately 50 μm up to 110 μm within 10 seconds (Figure 2). The pores remain dilated as long as the ultrasound is active but return to original size three hours after ultrasound cessation.

Figure 2: Pore dilation due to ultrasonic excitation.
The square waveform is the “ramming force” which pushes the drug into the enlarged pores. As the waveform switches from one to the other the potential for cavitation is minimised. By increasing the time on the square wave transmission we were able to obtain deeper drug penetration of the insulin within the skin.
A 30-second sawtooth-only waveform transmission at the start of the signal generation, known as skin priming, has the effect of dilating the pores. Thereafter the alternating signal engages, sequencing between sawtooth and square-wave transmissions, with no degradation of the insulin and no skin damage.
TRANSDUCER DESIGN
We found that conventional piezoelectric transducers could not develop the alternating waveform effect. No matter what electrical signal was given, they generated a sinusoidal wave, which is to be avoided in ultrasonic drug delivery.
A new approach with changes in the design and the material selection for the U-Strip transducers produced the Generation-5 transducer, which could convert the electrical waveform into a sonic waveform at the same wave shape, period, frequency and intensity.
The transducer’s mechanical force output will mirror exactly the electronic signal given to it from the ultrasonic driver circuit within the control device. An alternating waveform can be generated, consisting of any combination of primary and secondary waveform. For insulin delivery to the dermis, the sawtooth + square alternating waveforms work best.
TRANSDERMAL PATCH DESIGN
To solve the problems of electronically assisted transdermal delivery systems, to enable them to become more portable or wearable by the patient, and in consideration of conventional patch designs wherein drug contamination or denaturing may be caused through interaction with an adhesive or polymer component within the patch design, a new-patented two-part transdermal patch, Patch-Cap™ was developed. It is designed specifically for ultrasonic and other electronic drug delivery applications where a conventional patch is unsuitable due to its reliance of a drug/ adhesive mixture.
In the Patch-Cap (see Figure 3) an absorbent pad is used to store the drug until ultrasound, delivered from a snap-on transducer coupler, liberates the drug from the cap and onto the patient’s skin surface.

Figure 3: Use of an adhesive pad to store and release insulin. Elimination of adhesive.
The Transducer Coupler contains up to four miniature ultrasonic transducer elements and is powered by the re-usable U-Strip Ultrasonic Drug Delivery System. The Patch-Cap contains the drug, and is disposable. The current design holds up to 150 units of insulin, enough for a two-day supply for most diabetics using the U-Strip delivery system. The Patch-Cap is designed to be replaced every 24 hours.
Absorbent Pads to Contain the Drug
In reservoir, matrix and drug-in-adhesive versions of transdermal patches only a low drug concentration is possible. The delivery rate is often dependent upon the surface area of the patch. In the Patch-Cap the thickness of the absorbent pad can be varied to marry with the absorbency factor, so that more of the active drug can be contained within the fabric of the absorbent pad. For example a 1 cm2 of cellulosic pad can hold up to 12 times its weight in moisture at 1 mm thickness. The same pad thickness, but using a nylon pad holds only three times its weight. By varying the material used and altering the thickness the absorbent pad can be adjusted to meet a desired release rate and longevity, far exceeding that of conventional patches.
No Drug-Adhesive Contact
The use of adhesives that directly contact the drug is eliminated in this design. Adhesives may be used in the border of the Patch-Cap, but the drug-in-adhesive, matrix or reservoir designs are discarded in favour of an absorbent pad which is held in place in the cap by the use of an inner snap ring.
Ultrasonic Signal Emmitter-Skin Coupling
In conventional ultrasound systems a hydrogel is used to provide a coupling agent. The use of a gel-coupling agent could possibly interfere with and even contaminate an active drug substance liberated from the patch onto the skin surface. The PatchCap avoids the requirement for a coupling gel by using the liberated drug itself as the coupling agent to transmit the sonic signal from the transducer to the patient’s skin.
Low-Profile Patch

Figure 4: Low-profile Patch Cap with butterfly shaped backbone (7.5 cm across).
Initial Patch-Cap designs was somewhat bulky so continued development lead to a much smaller, more compact TDD, called the Low-Profile Trans-Insulin Patch, which was more easily worn by the patient. The backbone of the patch is butterfly shaped with wings containing an adhesive border to enable it to stick to the skin (Figure 4). The centre section of the patch holds the insulin, but the patch is designed so that no adhesive comes into direct contact with the insulin.
Dose Limiting Safety Feature
The U-Strip insulin TDD has a special on/off feature. Insulin is liberated from the patch by ultrasonic transmission and passes through a semi-permeable film which acts to retard the flow rate of the insulin and also acts as an on/off valve. It limits the maximum rate at which insulin can be released from the patch to no more than two units per minute, irrespective of ultrasound intensity, or the length of time the ultrasound is present. This top limit of dose control prevents over-dosing.
In addition the semi-permeable film will not permit insulin release from the patch until the ultrasound is active. No ultrasound, no delivery. This on/off valve function is therefore also a safety mechanism to prevent any extra insulin delivery after the controller switches the ultrasound off.
Delivery Pattern Upon the Skin

Figure 5: A filter at the bottom of the patch gives a dot pattern distribution of insulin on the skin, improving delivery.
To improve the speed of drug absorption upon liberation from the patch, the delivery pattern of the insulin is directed to enter the skin at the site of the skin pores. A filter at the bottom of the Trans-Insulin patch reduces the drug to miniature droplets which approximate the spacing for the skin’s pore structure. As a result the insulin is absorbed more completely into the skin and at a faster pace. See Figure 5, where the insulin is marked with a blue dye, and is more readily absorbed at the pore distribution sites.
The insulin droplet pattern approach reduced the quantity of insulin needed to be stored within the TDD and increased the speed of absorption into the skin. In clinical testing of the original design of the Patch-Cap it took five hours of constant ultrasound to reduce the glucose by just 40 points, compared with just 30 minutes for 87% of the volunteers tested using the device with the dot pattern.
DELIVERY RATES, DURATIONS AND SCHEDULES
The U-Strip® Desktop Unit is designed to provide fast glucose reduction for both excessively high starting glucose and for emergency situations. The portable device, which can be worn on a belt (Figure 7) or on the arm, is designed to deliver insulin at a rate of no more than 7 units/hr.
The recommended delivery rate for a 90 kg (200 lb) male for Lispro insulin is 15.230 units per eight hours, or 1.9-3.75 units/ hr. The delivery rate of the U-Strip Desktop Unit can be as high as 16.6 units/hour.
The U-Strip, holding 100 units or up to 150 units can provide 6.6 or 9.0 hours, respectively, under constant ultrasound. An intermittent activation schedule has been developed whereupon the device is activated for 15 minutes out of every hour and remains deactivated for the balance of 45 minutes of each hour for standard basal operations. Under this schedule, at the maximum liberation rate the patches would supply insulin for up to 36 hours. Since most Type-2 diabetics would not need more than 1.9 units/hr these patches could last more than three days (see Table 1).
| Patch designation | Load capacity | Liberation rate | Duration mad constant ultrasound | Duration max using standard +15/-45 delivery schedule |
| U-100 | 100 u | 15.1 u/hr | 6.62 hr | 26.43 hr |
| U-150 | 150 u | 16.6 u/hr | 9.03 hr | 36.01 hr |
Table 1: Table comparing delivery longevity from U-Strip devices with two different load capacities (desktop control unit)
One of the most prevalent problems with diabetes is high morning glucose. This is due to a slacking off of the insulin potency over the night from a standard injection therapy, and in the morning the liver can produce more glucose, in anticipation of the day’s events. A unique delivery schedule has therefore been developed using U-Strip whereupon insulin is pulsed from the patch for the first four hours. As shown in Table 2, under the “A” schedule the patch is set to deliver from 1.9 to a high of 7.65 units/hour for the first four hours, assuming an eight-hour sleep. For the two hours between hour four and hour six, the delivery rate ramps downward to ensure glucose does not drop too low during the night. Just before waking the U-Strip increases the insulin delivery to enable the patient to wake with the glucose level of a healthy non-diabetic. Glucose stability exceeded the glucose control variants of metformin, the most widely prescribed oral medicine for Type-2 diabetics.
| Patch designation | Load capacity | Insulin | Liberation rate at full U/S |
| U-150 | 150 u | Lispro R | A = 1.9 to 7.65 /hr capability for 1-4 hr |
| U-150 | 150 u | Lispro R | B = 1.2 to 5.125 /hr capability for 4-6 hr |
| U-150 | 150 u | Lispro R | C = 1.9 to 7.65 /hr capability for 6-8 hr |
Table 2: Three possible delivery schedules from U-Strip (mini control unit).
SAMPLE CLINICAL DATA
In one clinical trial, named HPT-6A, in volunteers given a meal immediately before treatment, the U-Strip system defeated the glucose spike that would normally occur post-meal. The post-meal application of Lispro insulin from U-Strip brought each volunteer to the range of healthy / normal in as little as 35 minutes. The plasma glucose in all volunteers dropped by 8-10 points in just the first five minutes of treatment. Additional trials are underway, including a 500 patient trial, before applying for regulatory approval. In over 200 Type-2 patients studied there have been no adverse events, with complete reduction and stabilisation of glucose levels at healthy normal range (85-110 mg/dl) from starting levels as high as 300 mg/dl.
Compared with an insulin pump (Figure 6) the U-Strip was just as effective in obtaining glucose control, except the U-Strip was totally non-invasive and can achieve the same results with far less delivered insulin. In these trials the efficiency of ultrasonically administered insulin was found to be 400% greater than pump delivered insulin in obtaining compatible glucose control. The bioavailability and pK values of ultrasonically delivered insulin are greater than that provided by insulin pumps.

Figure 6: Glucose reduction over 5hr – U-Strip compared with an insulin pump.
SUMMARY

Figure 7: The U-Strip System, comprising arm-mounted mini controller and patch
U-Strip is a transdermal delivery system capable of delivering large-molecule drugs through the skin, non-invasively. The company is presently developing an insulin patch aimed at Type-1 and insulindependent Type-2 diabetics (market potential 4 million patients in the US alone). The patient can wear the insulin patch product, in the form of a two-part transdermal drug delivery device, the Patch-Cap, powered by an ultrasonic delivery controller, during their daily routine (Figure 7). The device regulates the dosing of insulin in both basal and bolus delivery needs.
The use of a two-Part TDD solved many critical concerns limiting the use of transdermal patches in drug delivery applications, especially considering electronically assisted delivery systems.
REFERENCES:
- US Patents: 4,751,087; 5,209,879; 5,271,881; 5,455,342; 5,460,756; 6,908,448; and 7,440,798.
- Barrie-Smith N, Lee S, Kirk Shung K, Roy RB, Maione E, McElligott S, Redding BK, “Ultrasound-Mediated Transdermal Transport Of Insulin In Vitro Through Human Skin Using Novel Transducer Designs”. J Ultrasound Med Biol, 2003, Vol 29(2), pp 311-317.
- Mitragotri S, Blankschtein M, Langer R, “Ultrasound-Mediated Transdermal Protein Delivery”. Science, 1995, Vol 269, pp 850-853.
- Mitragotri S, Blankschtein M, Langer R, “Transdermal Drug Delivery Using Low-Frequency Sonophoresis”. Pharm Res, 1996, Vol 13(3), pp 411-420.
- Johnson ME, Mitragotri S, Patel A, Blankschtein M, Langer R, “ Synergistic Effects of Chemical Enhancers and Therapeutic Ultrasound on Transdermal Drug Delivery”. J Pharm Sci, 1996, Vol 85(7), pp 670-679.
- Kost J, Langer R, “Ultrasound-Medicated Transdermal Drug Delivery”, in “Topical Bioavailability, Bioequivalence and Penetration”, 1993, pp 91-104. Published by Plenum Press, (New York, NY, US).
- Mitragotri S, Edwards DA,
Blankschtein D, Langer R, “A Mechanistic Study of Ultrasonically-Enhanced Transdermal Drug Delivery”. J Pharm Sci, 1995, Vol 84(6), pp 697-706. - Johnson ME, Blankschtein D, Langer R, “Evaluation of Solute Permeation Through the Stratum Corneum: Lateral Diffusion as the Primary Transport Mechanism”. J Pharm. Sci, 1997, Vol 86(10), pp 1162-1172.
- Kost J, Mitragotri S, Gabbay RA, Pishko M, Langer R, “Transdermal Monitoring of Glucose and Other Analytes Using Ultrasound”. Nature Med, 2000, Vol 6(3), pp 347-350.
- Miyazaki S, Mizuoka H, Kohata Y, Takada M, “External control of drug release and penetration”. Chem Pharm Bull, 1992, Vol 40(10), pp 2826-2830.
- Kral LP (Editor), “World Book of Diabetes in Practice”, 1988, pp 160163. Published by Elsevier.
- Kanikkannan N, Singh J, Ramarao P, “In vitro transdermal iontophoretic transport of timolol maleate: effect of age and species”. J Controlled Release, 1999, Vol 59(1), pp 99-105.
- Zegzebski JA, “Essentials of Ultrasound Physics”, 1996. Published by Mosby (St Louis, MO, US).
- Stansfield D, “Underwater Electroacoustic Transducers”, 1990, pp 79-257. Published by Bath University Press (Bath, UK).
- Wilson OB, “An Introduction to Theory & Design of Sonar Transducers”, 1998, pp 89-108. Published by Peninsula (Los Altos CA, US).
- Shung KK, et al, “Principles of Medical Imaging”, 1992, pp 102-123. Published by Academic Press.
- Williams J, “A Fourth Generation of LCD Backlight Technology”. Application Note 65, 1995, pp 1-124. Linear Technology Corporation (Milpitas, CA, US).
- Agbossou K, Dion JL, Carijnan S, Abdelkrim M, Cheriti A, “IEEE Transactions on Ultrasonics”. Ferroelectrics & Frequency Control, 2000, Vol 47, pp 1036-1041.
- Wilking SL, Husberg ML, Ko CU, Wick SM, “Effect of Excipients on Physical Properties of Selected Acrylate, Polyisobutylene & Silicone Pressure Sensitive Adhesives Commonly Utilized in Transdermal Drug Delivery Systems”. Pharm Res, 1994, Vol 11, Suppl 226.
