Citation: Gallem T, “The eFlow ‘Closed System’ (CS) – A Novel Device Platform For Liquid Aerosol Drug-Device Combinations”. ONdrugDelivery Magazine, Issue 50 (Jun 2014), pp 13-16.
Thomas Gallem describes the design and development stages, including the incorporation of human-factors engineering and optimisation for elderly patients, of the company’s eFlow CS nebuliser, which uses a proprietary single-dose drug ampoule as an integral part of the nebuliser handset.
INTRODUCTION
Inhalation systems based on eFlow® Technology provide the benefit of short nebulisation time, silent operation and mobility for patients relying on frequent aerosol therapies. The eFlow CS device combines PARI Pharma’s perforated, vibrating membrane technology1 to generate liquid aerosols of controlled droplet sizes, with a proprietary blow-fill-seal (BFS) ampoule which can be opened solely in the device. Use of this single dose drug ampoule optimises dose uniformity,2 simplifies medication dispensing from the drug vial into the nebuliser and minimises potential for misuse, such as taking the wrong medication or the wrong dose.
In the first development stage, a functional prototype was built to evaluate the device performance in vitro, to draw interest from potential pharmaceutical partners, and to enable use of the eFlow CS (not customised at that stage) in clinical studies with their drug of interest. In the second stage, the device was further optimised to the specific requirements of the target user population of elderly COPD patients. Several usability studies have been performed which resulted in an iterative optimisation process to ensure that the target population is able to use the device safely and effectively.
DRIVERS FOR THE DEVELOPMENT OF eFLOW CS
The eFlow aerosol delivery platform3 was established to meet the versatile needs of patients and caregivers. Currently, as part of this platform, PARI Pharma offers two different categories of devices based on the eFlow technology for commercial use:

Figure 1: Altera® Nebuliser System with labelling on nebuliser handset and aerosol head indicating drug specific use.
- The open system platform for general use (eFlow® rapid in the EU, eRapid® in the US) consists of devices which received market clearance in the US via a 510(k) premarket notification (CDRH Guideline 784) and in the EU by CE marking. Similar in performance to traditional jet nebulisers but with significantly reduced nebulisation times, the intended use of these nebuliser systems comprises the administration of standard medications for inhalation as prescribed by the physician.
- The drug-specific eFlow devices (e.g. the Altera® nebuliser for Gilead’s inhaled antibiotic, Cayston® (aztreonam) for use in cystic fibrosis), which require a drug-specific 510(k) approval in US with an intended use restricted only to medications for inhalation that have been approved with the specific device.
For the latter, to indicate that the drug-specific device has to be operated with a particular drug, a mutually conforming branding and labelling concept was introduced. This comprises branding and labelling of the nebuliser system including the nebuliser handset and aerosol head (Figure 1) with a clear statement about the intended use on the packaging and in the instructions for use (IFU).
Although this branding concept has been successfully implemented, the fact that the nebuliser handset provides an open medication reservoir still leaves room for misuse. It was therefore the next logical step to develop a forward-looking device concept that would address this issue, adding value for PARI Pharma’s licensing partners.
A closer look at the handling procedures for existing nebulisers, which a patient needs to follow in order to take his/her daily inhalation therapy, revealed that many steps can impact successful therapy. Dose uniformity, for example, is influenced by the special care which a patient takes when dispensing his medication from the drug vial into the nebuliser reservoir. In addition, there are no lockout mechanisms in the nebulisers that can prevent the patient from choosing the wrong medication or dose. This might affect treatment safety, especially with advanced, highly efficient nebuliser systems.
To address this unmet need, the eFlow® CS device has been developed. It uses a proprietary single-dose drug ampoule as an integral part of the nebuliser handset. This specific ampoule is required to interface with the aerosol-generating membrane of the nebuliser handset during use. Opening the ampoule is possible only when the ampoule is inserted into and mated with the nebuliser handset.
FUNCTIONAL PRINCIPLES OF THE eFLOW CS DEVICE
The eFlow CS Ampoule
Besides its function as the primary packaging container for the liquid drug formulation, the ampoule of the eFlow CS is designed as an integral component of the nebuliser-handset assembly, enabling a unique drug-device interface. This defines a number of additional requirements, such as sufficient mechanical stability, precise ampoule geometry (particularly in the areas of the ampoule-nebuliser interface), and the ability to be produced in a large-scale manufacturing process.
A blow-fill-seal (BFS) process 7 was found to be best suited for this purpose and was finally chosen from the available options for production of the eFlow CS ampoule. A low-density polyethylene (LDPE) material was selected as it provides the required mechanical properties and, in addition, LDPE is widely-used for packaging of liquid medications for inhalation.
The specific design elements of the eFlow CS ampoule are described in Figure 2.

Figure 2: Specific design elements of the eFlow® CS ampoule.
The full cross-sectional view (Figure 2) visualises the closure plate (b) with the circular predetermined breaking line. This part of the ampoule is designed to break off along the edge of the plate, flip aside and rest in a defined vertical end position when the opening collar (Figure 3) and the ampoule are fully engaged. The protection rim (Figure 2, (a)) will prevent the ampoule from unintended opening. The chamber of the ampoule can hold fill volumes of 0.8-2.5 ml. The shell of the ampoule has a ring-shaped groove to mount the ampoule inside the medication cap or similar holding feature. When the ampoule is inserted into the nebuliser, a labelling tag remains visible so that the patient always knows which medication is filled (Figure 4).
Drug-Device Interface of the eFlow CS
The concept drawing in Figure 3 visualises the eFlow CS nebuliser handset (left) and the operating principle of the ampoule opening and medication feeding mechanism, including the eFlow CS aerosol head (1), the opening collar (2) and the ampoule (3).

Figure 3: Functional components of the eFlow® CS opening and medication feeding mechanism.
The core component for aerosol generation, the eFlow CS aerosol head (1), is similar to the one used in the commercially available eFlow devices (e.g. Altera®). Its peripheral portion (the blue ring-shaped part in Figure 3) was adapted to the requirements of the eFlow CS nebuliser handset whereas the vibrating centre portion remained unchanged. The opening collar (2) is essential for a reproducible ampoule opening and medication feeding process. It punches and opens the ampoule when both parts are fully engaged. The opening collar is integrated within the top of handset assembly. Upon opening of the closure plate the medication flows from the ampoule (3) through the lumen of the opening collar and comes into contact with the perforated membrane of the aerosol head from where it can be nebulised following activation.
The medication cap integrates the ampoule into the nebuliser. This cap interacts with the top of the handset part and enables drug loading and liquid feeding in two steps. First, the ampoule is inserted into the medication cap which then is attached to the nebuliser. While turning and closing the medication cap, integrated threads transfer the rotation into a linear motion of the ampoule relative to the opening collar. When the end position is reached, the system is primed for starting nebulisation.
For improved delivery efficiency during continuous nebulisation, the eFlow CS nebuliser handset also features a flow-optimised aerosol chamber with valves.5,6 Upon inspiration by the patient the inspiratory valve in the top of the handset opens allowing the inspiratory flow to entrain the aerosol generated into the chamber. Upon expiration the inspiratory valve closes and the expiration flow is diverted via the expiratory valve at the mouthpiece. During the expiratory phase, aerosol is continuously generated and collected in the chamber for delivery in the next inspiratory phase. Thus, aerosol losses are minimised and the delivery rate maximised.

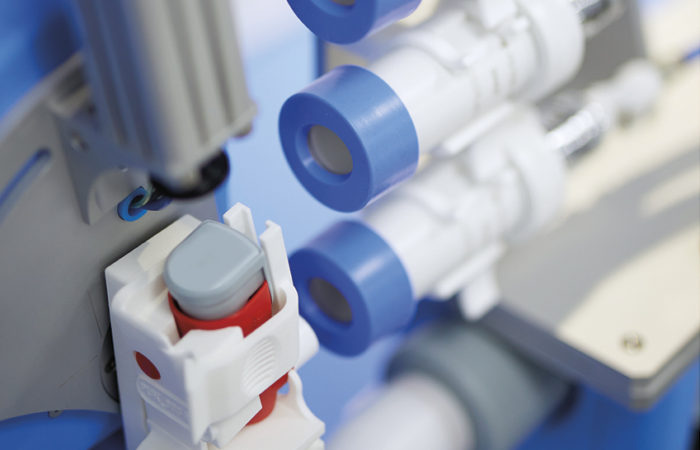
Figure 4: Functional prototype of the eFlow® CS nebuliser (before customisation).
To verify the performance of the novel device concept, a functional prototype (Figure 4) was built and tested in vitro. In order to retain flexibility with respect to subsequent optimisation and customisation for various clinical programmes, a modular preproduction tool for the eFlow CS ampoule was built for aseptic filling of investigational drug products suitable for fill volumes between 0.8-2.5 ml (HOLOPACK GmbH7).
The results of the design verification test exceeded most expectations.2 The residual volume remaining in the ampoule and opening collar at the end of a treatment is about 0.15 ml and virtually independent of the fill volume. Varying the holding angle of the eFlow CS nebuliser handset in a range of 20° forwards to 40° backwards from a horizontal oriented mouthpiece axis had no significant effect on the drainage properties and the total output, using isotonic saline. This was an important prerequisite for the required delivered dose consistency under typical handling conditions.
CUSTOMISING THE eFLOW CS FOR ELDERLY USERS (65+)
The first use of the eFlow CS functional prototype in a clinical study was in the third quarter of 2012. The preparation of the study devices made clear that some of the elderly COPD patients, especially those with age-related handicaps (e. g. visual, hearing and dexterity impairments), may struggle with using the device according to the IFU. Therefore, a series of user studies was planned and performed in order firstly to identify the use-related risks and secondly to optimise the device for the intended user population.
Following common best-practice rules for human factors engineering,9 this process started at an early stage of the device customisation by defining users, uses and use environments. The focus of the user studies was on use-related hazards and understanding the risks associated with them, and it followed a coherent plan to identify and address any human-factors issue. The IFU and the accompanying documents including the packaging were regarded as part of the user interface and therefore tested as thoroughly as any other part.
In alignment with the regulatory requirements as described in the Draft US FDA Guidance for Human Factors Engineering (HFE) and the International Standards ANSI/AAMI/IEC 62366 & ANSI/AAMI/ ISO 14971, an HFE file was created to document the user-study results and the iterative device improvements.
A first observational user study in the target population of elderly COPD patients aged between 65 and 80 revealed the most critical handling steps with the device. Due to the restricted physical and mental capabilities of the target population, even fairly simple handling steps like “open nebuliser top”, “remove medication cap” and “insert ampoule” could not be successfully finished by all participants (Figure 5). In addition, the rough handling observed during the user studies called for further improvement of the robustness of the device.

Figure 5: Critical handling steps identified in an early user study in elderly COPD patients.
Based on these findings, new design concepts were developed supporting more intuitive handling. In this device optimisation process all design elements that are relevant to the aerosol performance of the eFlow CS nebuliser handset, such as the medication feeding mechanism (Figure 3), the valves, the aerosol chamber and the aerosol head, had to remain unchanged.
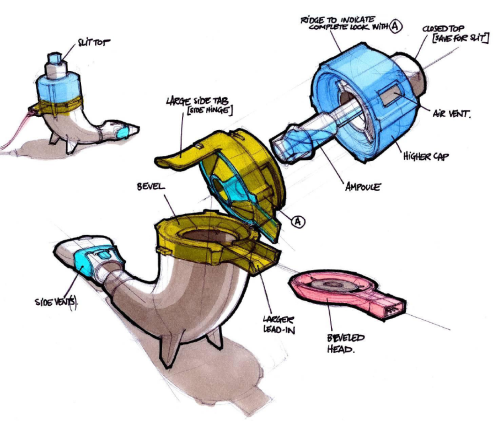
Several design concepts have been developed and evaluated and the one that best fulfils the new user-related requirements is depicted in Figure 6. Its main design features are:

Figure 6: Design concept of an optimised eFlow® CS device for elderly COPD patients.
- An improved ampoule that can only be inserted into the nebuliser in one way
- An enlarged and simplified medication cap that reduces the ampoule opening torque and provides a better grip
- A sideways nebuliser opening for improved aerosol-head accessibility and assembly
- A more robust interface for the connection cord adapter.
This design concept was transferred into a new eFlow CS device (Figure 7) which will be ready for use in a large, multicentre Phase III clinical study later in 2014. The robustness and ease of handling of the new design has been demonstrated by several usability studies and iterative design optimisation including intense design verification testing. The results of the pre-summative user study confirm that the issues identified in Figure 5 have been successfully addressed. External HFE specialists10 were involved in planning and conducting the user studies for the device optimisation process. Their support covered the whole range of HF activities including the recruitment of study participants to the point of the creation of the summative HF study report. In addition, most HF service providers offer access to an infrastructure to execute the user studies in a real life environment.
SUMMARY

Figure 7: eFlow® CS for elderly COPD patients (after customisation).
The novel eFlow CS inhalation device, an advanced, highly efficient nebuliser system, has been developed to improve treatment safety. It features an integrated, singledose BFS drug ampoule combined with a unique opening mechanism. Since the specific ampoule is required to operate the device, potential misuse, like choosing the wrong medication or filling the wrong dose, is minimised.
The integration of the ampoule with the device removes human errors from improperly adding the drug solution into the nebuliser while improving dose-uniformity and hygiene requirements.
Supported by a series of user studies, the design was optimised for the target user population of elderly COPD patients. The new design has been demonstrated to fulfil the technical requirements and to support intuitive handling.
REFERENCES
- Knoch M, Keller M, “The Customized Electronic Nebulizer: a New Category of Liquid Aerosol Drug Delivery Systems”. Expert Opin Drug Del, 2005, Vol 2(2), pp 377-390.
- Gallem T, Tservistas M, Uhlig M, Waldner R, Seemann S, Keller M, Knoch M, “Evaluation of an Ampoule- Based Nebuliser System Intended to Facilitate Accurate Dosing”, Proc Respiratory Drug Del Eur (RDD Europe), 2009, pp 341-244.
- Keller M, Knoch M, “Optimising Drug & Device Together for Novel Aerosol Therapies”, ONdrugDelivery Magazine, Issue 17 (Mar 2010), pp 12-16.
- Gallem T, Tservistas M, Waldner R, Loenner M, Knoch M, Keller M, “Assessment of the Influence of the Holding Angle on Drainage and Output Properties of a new Ampoule-Based Nebuliser System”. Proc Respiratory Drug Del (RDD), 2010, pp 713-718.
- Borgschulte M, Germer M, Hug M, Keller M, Knoch M and Stangl R, “Means to Optimize Drug Delivery from a Novel Electronic Inhaler”. Proc Respiratory Drug Del (RDD), 2004.
- Patent family based on German patent: DE 199 53 317, e.g. US 6,962,151.
- HOLOPACK Verpackungstechnik GmbH; www.holopack.de.
- US FDA Draft Guidance, “Applying Human Factors and Usability Engineering to Optimize Medical Device Design”. June 2011.
- http://IPAC-RS HF Webinar 2012, slide 9 www.ipacrs.com.
- Leslie E. Johnston, Senior Human Factors Engineer, Cambridge Consultants, Inc (Cambridge, MA, US).
Previous article
GENERIC PMDI PRODUCT DEVELOPMENT FOR THE US: KEY CONSIDERATIONSNext article
FORMULATION METHODS & SIZE REDUCTION FOR INHALERS