Citation: Copley M, “Improving the Realism and Relevance of Mouth-Throat Models for Inhaled Product Testing”. ONdrugDelivery Magazine, Issue 57 (Apr 2015), pp 32-37.
Mark Copley provides some background on mouth-throat models for OIP testing.
Last year’s announcement of US FDA funding to support the experimental assessment of different mouth-throat models for orally inhaled product (OIP) testing 1 draws attention to the recognised limitations of the standard US and EU Pharmacopoeias (USP/ Ph Eur) induction port used for cascade impaction (CI) measurements.
Primarily developed to meet requirements for a robust and simple test set-up for quality control (QC), this standard interface is a uniform right angled bend that fails to provide an accurate in vitro realisation of flow through the upper respiratory tract.2 This limitation is becoming increasingly important as the industry works towards better in vitro-in vivo relationships (IVIVRs) to support product development. During OIP development, better IVIVRs aid the faster commercialisation of efficacious products and the more secure demonstration of bioequivalence, in the case of generics.
The Alberta Idealized Throats (see Figure 1), adult and child (AIT and C-AIT respectively), were developed specifically to meet the need to simulate dose deposition behaviour in the mouth-throat more closely during OIP testing. This article presents experimental work demonstrating the performance of these accessories relative to the USP/Ph Eur induction port. The results indicate that the AIT and C-AIT deliver data that are more representative of measured deposition behaviour, suggesting that they have a role to play in improving IVIVRs. The article concludes with a survey of other strategies that are also helpful in securing more representative testing.
EVOLVING REQUIREMENTS FOR OIP TESTING

Figure 1: The AIT has a standardised, highly reproducible, human-like geometry offering robust performance across a broad range of flow rates.
Generally speaking, OIP testing is applied either:
- in QC – to verify that a product meets a defined specification ahead of batch release
- in R&D – to understand product behaviour better and optimise performance to deliver targeted in vivo drug deposition.
These two applications place different demands on an analytical test methodology. In QC the primary need is for simplicity, speed and sensitivity, since the goal is efficiently to assess samples against a specification. In contrast, during product development, the focus is on information gathering, to understand how to control product attributes to achieve the desired in vivo performance. Here accuracy and sensitivity alone do not guarantee success. Rather there is an additional need for the measured results to reflect in vivo performance and clinical efficacy, as far as possible.
The introduction of Quality by Design (QbD) brings this issue into sharper focus since a QbD approach is based on the knowledge-led manipulation of product parameters to deliver a defined Quality Target Product Profile (QTPP). To be useful within this context it is highly desirable that the results delivered by an in vitro method are closely representative of in vivo behaviour.
The particle size of aerosols emitted from an OIP directly influences deposition behaviour in the lung and is therefore a Critical Quality Attribute (CQA). CI testing is the primary particle sizing method used, principally because it measures the aerodynamic particle size distribution (APSD) of the active pharmaceutical ingredient (API) within a formulation, for the entire (collected) delivered dose. These features give the resulting data a high degree of relevance. Measurements are typically carried out using either an Andersen Cascade Impactor (ACI) or Next Generation Impactor (NGI), with the USP/Ph Eur induction port acting as the inlet to the impactor, to which the OIP is interfaced through the use of a suitable mouthpiece adapter.
The design intent of the induction port was to provide a uniform and robust representation of the human throat for QC testing. The accessory fulfils this purpose since it is easy to use and its simple geometry allows reproducible and repetitive drug recovery. However, the induction port is known to capture less of the delivered dose than would be deposited in the mouth-throat during routine OIP use by a patient.3,4 Though this limitation does not compromise QC testing it is a contributing factor to the poor IVIVRs that impact the relevance of testing in product development.
It should also be recognised that whilst a cascade impactor is not a lung model, and should not be considered as such, there is significant value in ensuring that the aerosol entering the cascade impactor is at least representative of the aerosol that enters the lungs, for the purposes of accurately measuring the APSD of the lung dose.
ALTERNATIVES TO THE STANDARD USP/PH EUR INDUCTION PORT
One fairly obvious alternative is a human throat cast.
A human throat cast provides a highly accurate representation of the mouth and throat, but unfortunately only for a single human subject. Because there are significant inter-subject differences in the geometry of the mouth and throat the use of different throat casts introduces an additional and substantial source of variability during testing. Furthermore there are a number of practical issues associated with the use of throat casts:
- their geometry is complex making them difficult to define dimensionally and manufacture reproducibly
- plastic-based materials typically used in their construction are prone to static, have poor durability and may release chemical extractables during analysis
- they are difficult to access internally for the purposes of drug recovery and dimensional verification
- they can be difficult to interface reliably with CIs.
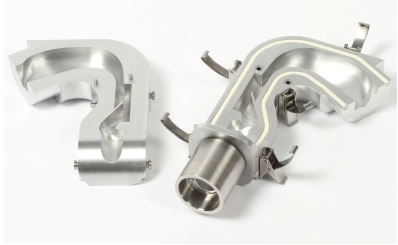
In summary then, human throat casts offer representative testing for a very closely defined patient group, but at the expense of practicality, while the standard USP/Ph Eur induction port offers practicality but is poorly representative of in vivo behaviour. The AIT is a rigorously researched alternative to these options, designed to combine the advantages of both.
The geometry of the AIT is the product of more than a decade of research at the Aerosol Research Laboratory of Alberta (University of Alberta, Canada) and was developed using an extensive database of computed tomography (CT) scans and reviews of anatomical texts. Today the AIT is a commercial product, precision manufactured to extremely close tolerances and designed to interface with a wide range of cascade impactors. Manufactured in metal it has a highly reproducible, human-like geometry which delivers performance that is validated against clinical data across a broad range of flow rates.3, 4, 5 Following successful trials with the adult AIT 3, 4, 6 a child version has recently been introduced, to enable the more representative testing of products for paediatric use. The geometry of this accessory is based on CT upper airway data from nine children aged six to fourteen years.7
The following experimental studies demonstrate the performance of the AIT/C-AIT, contrasting it with that of a standard USP/ Ph Eur induction port, and show how these accessories provide more accurate information for OIP development.
CASE STUDY 1: A COMPARATIVE TRIAL OF THE AIT AND USP/PH EUR INDUCTION PORT
To compare the performance of the AIT with that of the USP/Ph Eur induction port, APSD measurements were made for two different commercially available inhaler formats: a pMDI (active ingredient salbutamol sulphate(SS)) and a DPI (active ingredient formoterol fumarate).6
Full resolution CI measurements were made using an NGI, equipped with either the AIT or USP/Ph Eur induction port. In accordance with pharmacopoeial test specifications the pMDI was tested at a flow rate of 30 L/min and the DPI at a test flow rate of 60 L/min. All stages of the NGI and the AIT were coated with silicone oil applied in n-hexane solution (1wt%/v), for all measurements, but the USP/Ph Eur induction port was left uncoated, in line with standard practice. A pre-separator was incorporated between the inlet (AIT or induction port) and CI for DPI testing.
| USP/Ph Eur Induction Port | AIT | USP/Ph Eur Induction Port | AIT | |||||||
| Stage | Mean | SD | Mean | SD | Stage | Mean | SD | Mean | SD | |
| T/MP 1 2 3 4 5 6 7 MOC |
54.2 2.9 1.8 4.0 16.0 14.2 38.0 0.7 0.5 |
1.6 0.6 0.1 0.3 1.9 1.5 0.6 0.2 0.1 |
66.8 1.1 0.7 2.2 12.7 15.5 4.3 0.7 0.5 |
5.1 0.2 0.1 0.6 2.0 0.9 0.5 0.1 0.1 |
T/MP Preseparator 1 2 3 4 5 6 7 MOC |
1.4 4.3 0.7 1.0 1.2 1.1 0.4 0.1 0.1 0.0 |
0.2 0.2 0.1 0.1 0.1 0.1 0.0 0.1 0.0 0.0 |
3.2 3.4 0.3 0.7 1.1 1.0 0.4 0.1 0.1 0.0 |
0.2 0.2 0.0 0.0 0.1 0.0 0.0 0.0 0.1 0.0 |
|
| TOTAL FPD FPF GSD MMAD |
98.0 37.3 38.0 1.9 2.5 |
3.6 2.6 1.4 0.2 0.1 |
104.4 34.8 33.4 1.6 2.2 |
8.4 3.3 1.3 0.0 0.1 |
TOTAL FPD FPF GSD MMAD |
10.2 3.2 31.0 2.2 3.5 |
0.3 0.1 0.8 0.1 0.1 |
10.4 3.0 28.4 1.9 3.1 |
0.3 0.2 1.3 0.0 0.0 |
|
Table 1: Summary data for the pMDI (left) and the DPI (right) for the USP induction port and AIT. T/MP = throat/mouthpiece. Values are reported as µg/actuation, and the derived metrics are based on total emitted mass/actuation from the inhaler. MMAD is reported in µm.
Each measurement was conducted six times, resulting in 24 separate APSDs. The results are summarised in Table 1 which includes averaged profiles for distribution of the API (mean ±1 SD) across the collection plates of the CI, and in the throat and inhaler mouthpiece. These data were used to generate the standard particle size metrics used to characterise OIPs which include:
- fine particle dose (FPD) – the amount of drug which would be expected to reach the deep lungs on the basis of aerodynamic particle size (mg or µg)
- fine particle fraction (FPF) – the fraction of the delivered dose that would be expected to reach the deep lungs on the basis of aerodynamic particle size (%)
- mass median aerodynamic diameter (MMAD) – the particle aerodynamic diameter below which 50% of the particle population lies, on the basis of drug mass (µm)
- geometric standard deviation (GSD) – a measure of the breadth of the generated APSD.
An upper size limit of 5 μm was used for the calculation of FPD and FPF, which were based on the total dose emitted by the OIP into the inlet. All calculations were carried out using CITDAS V3.10 software (Copley Scientific, UK), assuming the APSD to be uni-modal and log-normal.
The results show that for both inhalers the AIT captures more of the emitted dose than the USP/Ph Eur induction port, thereby reducing the mass of drug entering the NGI. This observation echoes those reported previously for the AIT,3, 8 verifying its performance and potential value.
Furthermore, based on a previous study in which both the USP/Ph Eur induction port and the AIT internal geometry were coated,3, 4 this improved performance can be safely attributed to the geometry of the AIT rather than the applied coating.

Figure 2: Cumulative aerodynamic particle size data for the pMDI and DPI based on impactor sized mass for the USP/Ph Eur induction port and AIT.
Figure 2 shows the data as cumulative APSDs based on NGI-sized mass. The NGIsized mass is considered to be the portion of the dose that exits the induction port or throat and deposits on stages (and final filter) of the CI, having a particle size upperboundary defined by the cut-off diameter of the preceding stage. This normally results in omitting the drug mass collected on the first stage of the impactor.
These plots show that the effect of the AIT extends beyond simply the amount of dose captured. For the pMDI, use of the AIT shifts the APSD to finer sizes across the entire sized range, a trend summarised by an observed increase in FPF of approximately 8%, when only considering the impactor-sized mass. The associated reduction in MMAD is 2.5 ± 0.1 μm to 2.2 ± 0.1 μm and there is also an observable narrowing of the GSD from 1.9 ± 0.2 to 1.6 ± 0.0. Similar observations have also been reported elsewhere.9
The same trends are observed with the DPI. Here the increase in FPF, based on impactor-sized mass alone, is approximately 10% and there is an associated decrease in MMAD from 3.5 ± 0.1 μm to 3.1 ± 0.1 μm. GSD narrows from 2.2 ± 0.1 to 1.9 ± 0.0.
In summary, the AIT collects more of the emitted dose than the USP/Ph Eur induction port, which is known to underestimate mouth-throat deposition, suggesting that the AIT produces more representative data. However, the results also suggest that the AIT does not retain all particle sizes to an equal extent, but rather has a greater influence on the larger particles emitted by either inhaler.
CASE STUDY 2: ASSESSING THE PERFORMANCE OF THE C-AIT

Figure 3: Test set-up for evaluation of the performance of the C-AIT showing NGI, C-AIT and pMDI.
In a second experimental study the performance of the C-AIT was compared with that of the USP/Ph Eur induction port using two commercially available pMDIs of the same type (active ingredient SS).10 Generally speaking DPIs are less readily used for the treatment of paediatric patients, with MDIs the more common choice. The test set-up used (see Figure 3) was closely similar to that described above but a test flow rate of 15 L/min (±5%) was selected. Testing at 15 L/min is more representative of the inhalation characteristics of a paediatric patient and there is archival calibration data for the NGI at this air flow rate.11
Whilst it could be argued that, in the clinical situation, a small child would likely have been prescribed a valved holding chamber (VHC) for use with their pMDI, a VHC would have retained much of the coarse component of the dose from the inhaler, preventing it from reaching the inlet of the C-AIT. The inclusion of a VHC was therefore considered inappropriate, since the purpose of the study was to characterise the performance of the C-AIT alone.
Details of the test programme, which involved the use of multiple analysts and devices, are shown in Table 2. Each test measurement was the result of ten actuations of the inhaler with each actuation process involving a five second shake and a two second actuation followed by a five second hold, prior to removal of the device for the next test.
| Analyst | |||
| Test | Device | USP/Ph Eur Induction Port | C-AIT |
| 1 2 3 |
Device 1 | Analyst 1 | Analyst 2 |
| 4 5 6 |
Device 2 | Analyst 2 | Analyst 1 |
Table 2: Test programme for comparative testing of the C-AIT and USP/Ph Eur binduction port which involved two devices and two different analysts.

Figure 4: Deposition profiles for each stage of the NGI including the inlet for the USP/Ph Eur induction port and C-AIT measured at 15 L/min. Error bars denote max/min range of data.
Figure 4 shows the measured mass deposition profiles for the inlet and each stage of the NGI, based on the total mass/actuation emitted during testing.

Figure 5: Cumulative mass-weighted APSDs for pMDI-delivered SS for the USP/Ph Eur induction port and C-AIT.
The bulk of the SS dose was recovered from the inlet in either case, regardless of which analysts carried out the measurement and which device was used. However, as with the AIT, significantly more of the dose deposits in the C-AIT than in the USP/Ph Eur induction port; 82.4 ±1.6% compared with 67.4 ±2.1%. Both of the devices tested delivered similar results.
Figure 5 shows cumulative mass-weighted APSDs for the two inlets and includes data from both devices. These results confirm that the C-AIT, like the AIT, results in a small but discernible shift in the APSD to finer particle sizes, when compared with the USP/Ph Eur induction port. This observation is highlighted by the summary data in Table 3 which shows a statistically significant reduction in MMAD attributable to the use of the C-AIT; a shift in MMAD from 2.6 µm to 2.4 µm. The change is reflected in a corresponding reduction in FPF (based on delivered dose) when the C-AIT is used; 15.6% compared with 28.0% with the USP/Ph Eur induction port. GSD remains largely unchanged.
| Measure | USP/Ph Eur Induction Port | C-AIT |
| MMAD (µm) | 2.6 ± 0.1 | 2.4 ± 0.1 |
| GSD | 1.77 ± 0.04 | 1.81 ± 0.16 |
| FPF<5.0µm (%) | 28.0 ± 1.2 | 15.6 ± 1.6 |
| FPM<5.0µm (µg/actuation) | 28.2 ± 2.1 | 16.0 ± 1.3 |
Table 3: APSD metrics for the C-AIT and USP/Ph Eur induction port (Mean ± SD).
In summary the C-AIT, like the AIT, captures more of the emitted dose and preferentially retains coarser particles, inducing a small but significant shift in the MMAD. Interestingly the magnitude of the shift in MMAD to finer sizes was smaller for the C-AIT than for the AIT, 7% (from 2.6 µm to 2.4 µm) relative to 16% (2.5 µm to 2.2 µm). This difference may be attributable to the different flow rates applied during testing, and could suggest that the inability of the USP/Ph Eur induction port to mimic actual mouth throat deposition behaviour becomes more pronounced as turbulence in the respiratory tract increases.
THE BIGGER PICTURE

Figure 6: An optimised test set-up for procuring good IVIVRs in APSD testing of OIPs.
While the focus on a more anatomically correct inlet for OIP testing is important, other features of OIP testing also call for some refinement to meet the goal of better IVIVRs. A prime example is the inhalation profile applied during APSD measurements.
In standard CI testing (for DPIs) the applied inhalation profile is simply a square wave profile: an almost instantaneous on/off switch, taking the flow rate from zero L/min to a pre-determined, constant value for a short duration and back to zero L/min again. This is achieved through the use of a timed, rapid-acting solenoid valve in conjunction with a vacuum pump. This approach, developed to be compatible with the method of operation of cascade impactors (which are designed to work under constant flow rate conditions), clearly does not reflect the capabilities of a typical patient. It is, however, like the standard USP/Ph Eur induction port, highly suitable for QC testing due to its simplicity and reproducibility.
During product development the broader requirement is to assess how the patient’s inhalation profile impacts the success, or otherwise, of drug delivery and to what extent these profiles differ from those applied during routine testing. Consideration should be given to:
- the total volume inhaled
- the shape of the profile, which may not be uniform or symmetrical
- the peak flow achieved
- the rate of acceleration of the flow during the initial ramp up, which may be critical to aerosolisation of the dose (especially for passive DPIs) during the dose emission phase.
The commercial availability of cost-efficient breath simulators (exemplified by the BRS range from Copley Scientific) allows researchers to apply more representative inhalation profiles during OIP testing. To enable CI measurements simultaneously under constant flow rate conditions these breath simulators are applied in combination with a mixing inlet (see Figure 6). With a mixing inlet the flow rate applied through the OIP can be independently varied to allow application of realistic inhalation profiles (as perhaps measured in clinic) whilst the flow rate through the CI is maintained at a constant flow rate to deliver calibrated performance.12
With this test set-up the performance of an OIP can be assessed over a broad range of realistic inhalation profiles, in a way that is entirely consistent with the application of QbD. It becomes possible to assess the sensitivity of drug delivery to the inhalation strength of the patient for example, and/or specifically to test a product for a certain patient group with an atypical inhalation profile. Furthermore this set-up also enables the more robust demonstration of in vitro bioequivalence since it can be shown that the performance of a generic mirrors that of a reference inhaled drug product over a range of realistic inhalation profiles, not just a single square-wave profile.
A multi-faceted approach to the refinement of OIP testing is clearly critical as the industry works towards better IVIVRs. More anatomically correct representation of the mouth-throat is one part of the solution; more accurate simulation of the inhalation profile is another. In combination these refinements substantially enhance the value of in vitro testing, making it a far more relevant tool for the development of new and generic OIPs.
REFERENCES
- grants.nih.gov/grants/guide/rfa-files/RFA-FD-14-022.html
- Mitchell J, Nagel MW, “Cascade Impactors for the Size Characterization of Aerosols from Medical Inhalers: Their Uses and Limitations”. J Aerosol Med, 2003, Vol 16(4), pp 341-377.
- Zhang Y, Gilbertson K, and Finlay WH, “In vivo-in vitro comparison of deposition in three mouth-throat models with Qvar® and Turbuhaler® inhalers”. J Aerosol Med, 2007, Vol 20(3), pp 227-235.
- Weers J, et al, “In Vitro-In Vivo Correlations Observed With Indacaterol-Based Formulations Delivered with the Breezhaler”. J Aerosol Med Pulmonary Drug Delivery, 2015 (in press).
- Grgic B, Finlay WH, Heenan A F, “Regional aerosol deposition and flow measurements in an idealized mouth and throat”. J Aerosol Sci, 2004, Vol 35, pp 21-32.
- Copley M, Mitchell J, Solomon D, “Evaluating the Alberta throat: an innovation to support the acquisition of more clinically applicable aerosol aerodynamic particle size distribution (APSD) data in oral inhaled product (OIP) development”. Inhalation, 2011, Vol 5(4), pp 12-16.
- Golshahi L, Finlay WH, “An idealized child throat that mimics average pediatric oropharyngeal deposition”. Aerosol Sci Tech, 2012, Vol 46(5), pp i-iv.
- Watkins A, Gerrish T, Childerhouse N, “Comparative Performance of Dry Powder Inhalers Assessed Using a Commercially Available Model of the Upper Human Respiratory Tract”. Proceedings of Respiratory Drug Delivery Conference, 2012, pp 877-882.
- Poonam S, Fazel M, Stein SW, Myrdal PB, “Formulation Effects on Differential Throat Deposition for pMDIs with USP Inlet and Alberta Throat”. Proceedings of Respiratory Drug Delivery Conference, 2014, pp 631-635.
- Copley M, Parry M, Solomon D, Mitchell J, et al, “Comparison Between In Vitro Performance of Child ‘Alberta’ Idealized Throat and Ph.Eur./USP Induction Port for the Delivery of Salbutamol Sulfate Inhalation Aerosol by Pressurized Metered Dose Inhaler”. Inhalation Magazine, April 2015, Vol 9 (2).
- Marple VA, Olson BA , Santhanakrishnan K, Mitchell JP, Murray SC and Hudson-Curtis BL, “Next generation pharmaceutical impactor (a new impactor for pharmaceutical inhaler testing)—Part III: Extension of archival calibration to 15 L/min”. J Aerosol Med, 2004, Vol 17(4), pp 335–343.
- Casaro D, Bramilla G, Pasquali I, Sisti V, “In Vitro Aerosol Performances of NEXThaler Using Representative Inhalation Profiles from Asthmatic Patients”. Proceedings of Respiratory Drug Delivery Conference, 2014, pp 375-380.