


To Issue 188
Citation: Powell J, “De-Risking Post-Market Change Through Pilot Production”, ONdrugDelivery, Issue 188 (Jul 2026), pp 24–28.
Jon Powell explores how pilot production, delivered through integrated design, development and manufacturing capabilities, can be used to de-risk change in commercial-scale drug delivery devices, highlighting how such approaches can improve confidence in decision-making while reducing overall time and cost.
Managing change in drug delivery device manufacturing post launch is inherently challenging. Whether driven by regulatory requirements, issues with an existing on-market device, supply chain disruption or design evolution, even small modifications can introduce significant risk to product quality, cost and supply continuity. These challenges are compounded by the practicalities of generating statistically meaningful data from prototype designs without disrupting established, high-volume manufacturing operations.
“AS PRODUCTION INCREASES FROM HUNDREDS TO MILLIONS OF UNITS, VARIABILITY IN MATERIALS, PROCESSES AND REAL-WORLD USE CONDITIONS CAN REVEAL PREVIOUSLY UNOBSERVED BEHAVIOURS.”
WHAT DRIVES CHANGE IN DRUG DELIVERY DEVICES?
Even the most comprehensive design verification programmes cannot always accurately predict all failure modes that may emerge once a product is deployed at commercial scale. As production increases from hundreds to millions of units, variability in materials, processes and real-world use conditions can reveal previously unobserved behaviours. In addition to on-market performance considerations, manufacturers must also respond to external and internal drivers, such as:
- Regulatory updates
- Material obsolescence
- Supplier changes
- Cost optimisation initiatives.
Collectively, these factors make change management an essential element in the lifecycle of successful combination products. However, implementing changes without disrupting supply presents a significant challenge – the commercial justification often requires data that can only be gained by transitioning from small numbers of lab-built prototypes to thousands of devices produced using representative manufacturing processes.
While guidance such as ISO 20069:2019 “Guidance for assessment and evaluation of changes to drug delivery systems” provides a framework for assessing and documenting changes, it offers limited direction regarding exactly how to generate the representative data efficiently without impacting validated production lines.
A COMMON CHALLENGE
Consider an on-market drug delivery device that is currently being manufactured at scale. The production system to make and assemble such a device will be highly optimised. Material handling, in-process quality controls, final packaging, labelling – every step will be designed to reduce variation and ensure quality.
If such a device experienced an issue post-launch, the impact on the manufacturer could be enormous. The decision on how to proceed has significant consequences and could potentially trigger an intervention by the US FDA, the EMA or other regulatory bodies. This is reflected in the number of recalls and corrections reported by the FDA, underlining that the ability to implement changes to marketed products in a controlled way is a strategic need for manufacturers.
Examples from infusion and syringe-based drug delivery systems help to illustrate this challenge. Table 1 presents a selection of recent product recalls and corrections affecting this class of devices. Whilst the specific failure mechanisms differ, the examples highlight recurring challenges associated with fluid handling and sensing functions, such as leak paths and occlusion detection.
| Device | Failure Mode | Patient Risk | Date | Remediation |
|
Cardinal Health Monoject Luer-lock syringes |
Recognition, compatibility and pump performance issues when used with syringe pumps and patient-controlled analgesia pumps | Overdose, underdose, delay in therapy and delays in occlusion alarms | March 2024 | Recall of specific product |
|
B. Braun Infusomat Space Large Volume Pump |
On certain models, occlusion alarm may sound when no occlusion exists | Interrupted or failed delivery of medication or fluids | September 2023 | Correction of occlusion pressure sensor |
|
Fresenius Kabi Ivenix Infusion System |
Fluid leak that causes damage to the electrical system | Delay or interruption to treatment |
March 2023 | Urgent device recall letter sent to customers |
|
Eitan Medical Sapphire Infusion Pumps |
Failure to detect air in line when running on battery power | Risk of serious injury or death from air embolism |
September 2023 | Recall and customer notification, software update |
Table 1: Excerpt of recent product recalls/corrections affecting infusion and syringe-based drug delivery systems.1
Design modifications to address issues such as these require large data sets to generate sufficient statistical confidence that the issue has been resolved; where an issue is not fully understood or only occurs on an infrequent basis, this can potentially entail tens of thousands of units. The requirement for high numbers of finished devices exposes a gap in available manufacturing options:
- Volumes too high for conventional prototyping approaches
- Volumes too low, and timelines too short, to engage commercial-scale CMOs
- Existing production lines may not accommodate the design without significant disruption
This scenario reflects a common industry challenge, where development teams must balance two competing priorities: minimising change to fit with existing manufacturing capabilities versus allowing sufficient design freedom to maximise the likelihood of technical success.
CONTRACT MANUFACTURING CAN BE INFLEXIBLE
In conventional outsourcing models, CMOs are typically optimised for either low-volume engineering support or stable, high-volume commercial manufacture. Small-scale engineering workshops prioritise flexibility and rapid iteration, whereas production facilities are designed around efficiency, repeatability and validated processes (Figure 1). Projects that sit between these two models can create significant operational tension.
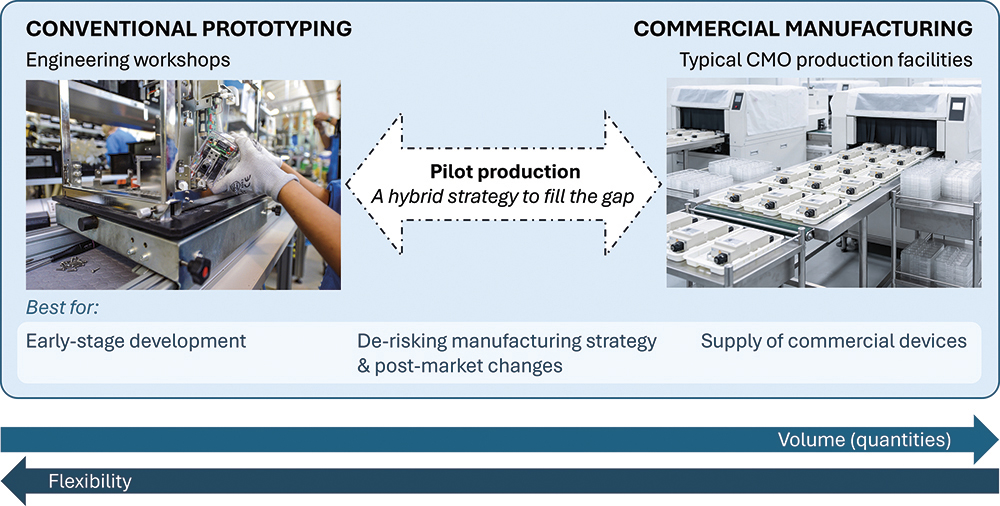
Figure 1: Typical device manufacturing models are optimised either for early-stage design and development or high-volume commercial manufacturing. Alternative models, such as pilot production, bridge this gap by combining the flexibility of engineering workshops with the repeatability and rigour of commercial production facilities.
In the case of drug delivery systems, the challenge is often amplified by the combination of bespoke automation, tight tolerances and sub-assemblies that contain both rigid and compliant parts. Even relatively small engineering programmes may require dedicated fixtures, custom tooling, automation development and specialised operator training. These investments can be difficult to justify when production volumes remain limited and product designs are still evolving.
Furthermore, these engineering builds often involve a high degree of uncertainty. Device configurations may change frequently, process parameters may still be under investigation and build schedules can fluctuate as development priorities evolve. For a CMO operating under conventional production metrics, such variability can disrupt factory planning, reduce equipment use and negatively impact operational efficiency.
There is also an economic challenge. Low-to-medium-volume engineering programmes rarely achieve the economies of scale associated with high-volume commercial manufacture, yet they may still demand significant engineering oversight and quality infrastructure. As a result, the commercial model can become unattractive for both the client and the manufacturing partner.
Many CMOs now advertise “Design” as a differentiator – spawning the initialism CDMO – offering design services as well as more traditional manufacturing services. However, as design is often not a core skill for these companies, they can leave clients with a design that only works with their in-house manufacturing approach, or where the IP rights no longer lie with the client.
For these reasons, many organisations may benefit from dedicated pilot production environments operating outside of conventional commercial manufacturing structures, providing a more effective route for executing complex flexible manufacturing.
CONVENTIONAL PROTOTYPING LACKS RIGOUR
Traditional prototyping is typically focused on evaluating functional concepts and demonstrating technical feasibility. Prototype devices are often produced in small quantities using flexible, low-volume methods that prioritise speed and adaptability over repeatability. These builds are valuable during early-stage development, where the objective is to assess usability, confirm mechanical principles or explore initial design architectures. However, prototypes are rarely manufactured under conditions representative of commercial production – as a result, they may not fully reveal the interactions between product design, automation strategy and manufacturing variability.
“RATHER THAN SIMPLY PROVING THAT A DEVICE CAN FUNCTION, PILOT MANUFACTURING AIMS TO DEMONSTRATE THAT IT CAN BE ASSEMBLED REPEATEDLY, EFFICIENTLY AND ROBUSTLY UNDER PRODUCTION REPRESENTATIVE CONDITIONS.”
Pilot manufacturing occupies a different position within the development pathway. Rather than simply proving that a device can function, pilot manufacturing aims to demonstrate that it can be assembled repeatedly, efficiently and robustly under production-representative conditions. This includes consideration of automation compatibility, process capability, quality inspection and operational throughput. The parts themselves are often manufactured by representative processes, such as injection-moulded plastic housings rather than 3D-printed parts.
This distinction is important because many challenges associated with drug delivery systems emerge only when products are built at scale. Tolerance accumulation, fixturing behaviour and automation interactions may appear manageable during low-volume prototyping but can become significant risks during industrialisation. By bridging the gap between prototyping and commercial manufacturing, pilot production enables engineering teams to identify and resolve these issues earlier in development, reducing industrialisation risk and supporting more robust product and process designs.
WHY EXISTING PRODUCTION LINES MAY NOT ACCOMMODATE DESIGN CHANGES
Many manufacturing systems for drug delivery devices rely on bespoke automation, tightly controlled tolerances and carefully sequenced assembly operations, specifically developed for a defined product configuration. Even relatively small design modifications, such as changes to component geometry, material behaviour or assembly orientation, can have cascading effects across the production process.
In automated systems, manufacturing equipment is often programmed around precise assumptions regarding part position, stiffness, insertion forces and component interactions. A seemingly minor design change may therefore require reconfiguration of robotic motion paths, vision system parameters, fixturing, feeding systems, inspection methods or a combination thereof. In some cases, the modification can introduce variability that existing automation is simply unable to accommodate reliably.
These challenges are particularly acute in assemblies containing both rigid and compliant parts. Elastomeric tubes, adhesives or soft materials may behave differently during automated handling when adjacent components are modified, creating interactions that only become apparent at production scale. For example, a section of tubing may curl in one direction 98% of the time based on how it is presented. The low occurrence of the alternative behaviour means it may not be observed in small sample sizes, leading to assumptions being made during automation development that later prove unreliable.
Importantly, commercial manufacturing lines for medical and combination products are usually validated environments operating under strict quality and regulatory controls. Any significant modification to equipment, tooling or process parameters may trigger formal change control activities, required revalidation and production downtime. For manufacturers supplying commercial products, this introduces both operational risk and potential supply chain disruption.
As a result, manufacturers are often reluctant to trial experimental designs directly on operational manufacturing lines, particularly where product demand remains high. This is where pilot production, as a hybrid of prototyping and commercial manufacturing, can provide a practical alternative. By replicating critical manufacturing operations outside the commercial environment, it allows design changes to be evaluated under production-representative conditions without interrupting ongoing supply, nor compromising validated manufacturing systems.
“A TARGETED APPROACH CAN BE ADOPTED TO BALANCE FIDELITY WITH FLEXIBILITY AND COST.”
DEVELOPING A HYBRID MANUFACTURING STRATEGY
Replicating the full complexity of the existing high-volume manufacturing system when conducting pilot manufacturing is usually neither practical nor necessary. Instead, a targeted approach can be adopted to balance fidelity with flexibility and cost.
This hybrid strategy, illustrated in Figure 2, involves:
- Mapping the device production process flow
- Identifying critical-to-quality and critical-to-function process steps
-
Assessing risk and applying suitable mitigations so that each of these steps is replicated using appropriate technology, for example:
– A needle insertion step that requires precise needle alignment (high risk) may require a controllable and repeatable automated system, such as a Selective Compliance Articulated Robot Arm
– Non-critical processes (low risk) could be conducted using manual or semi-automated methods.
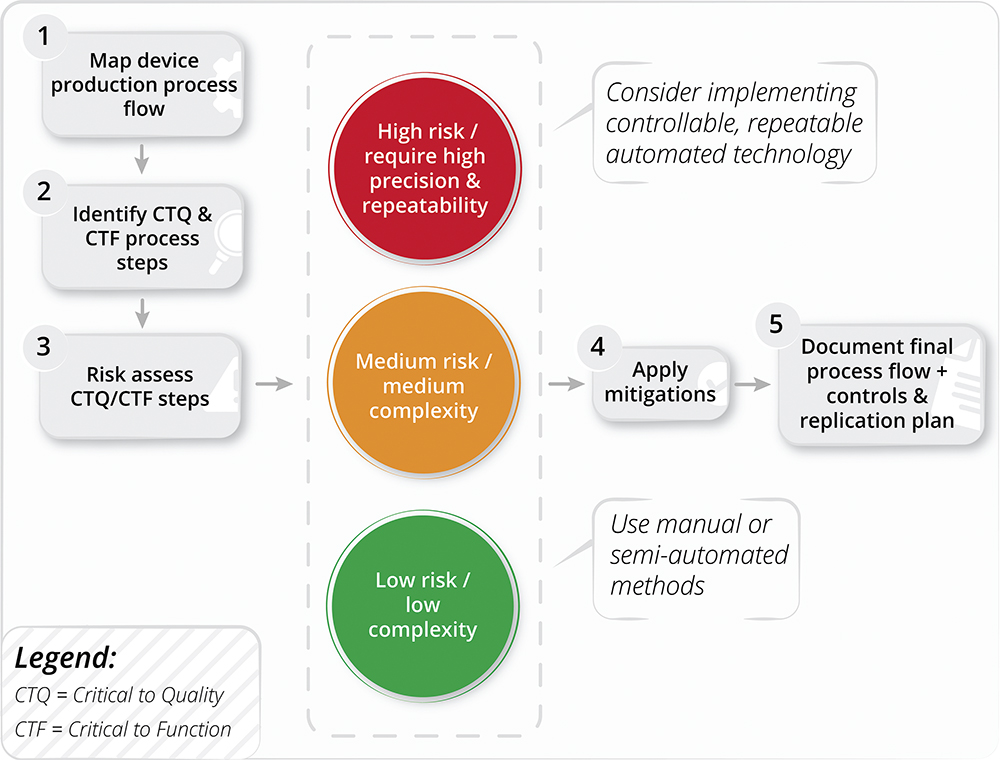
Figure 2: A hybrid manufacturing strategy used in pilot production to achieve a suitable balance between flexibility (allowing modifications) and fidelity (representative of commercial-scale processes).
As the pilot production system will be operating at a slower rate than a commercial line, a flexible approach to labour organisation and work balancing can mitigate uncertainties in the new, untested line. Even when simulating the new line with digital tools, the pinch points in production flows may not be known without running the system. The use of adaptable fixturing and work-in-process storage, which allows stations to build up inventories, is recommended to cope with these unknowns.
Additionally, it may be possible to redeploy equipment from the existing production lines to maintain process fidelity without incurring unnecessary cost. These valuable pieces of process equipment may be unused spares or repurposed from obsolete lines. However, due care and attention must be observed when bringing them online – they may have different voltages, require repair or maintenance or need production documentation to be translated from other languages.
IMPLEMENTATION AND OUTCOMES
The resulting pilot production line should incorporate a combination of approaches that can be designed and implemented rapidly:
- Automated assembly cells for critical processes
- Manual and fixture-based operations for non-critical steps
- Integrated inspection and functional testing capabilities.
“TO GIVE A REAL-WORLD EXAMPLE THAT PUTS THIS INTO CONTEXT, A PILOT PRODUCTION SYSTEM SUCH AS THIS WAS DESIGNED, BUILT AND OPERATED WITHIN A 12-WEEK TIMEFRAME, INCLUDING BOTH FACTORY ACCEPTANCE TESTING AND SITE ACCEPTANCE TESTING.”
To give a real-world example that puts this into context, a pilot production system such as this was designed, built and operated within a 12-week timeframe, including both factory acceptance testing and site acceptance testing. This enabled rapid deployment into an engineering production environment while design activities continued in parallel. In total, more than 14,000 devices were manufactured across seven design variants. These units supported:
- Engineering performance evaluation
- Accelerated ageing studies
- Ongoing engineering verification testing to prove functional performance.
The pilot production approach therefore provided both the scale and fidelity required to support robust, data-driven decision making.
CONCLUSION
For established drug delivery devices, the pressure to change can be driven by performance data, regulatory evolution, supply chain disruption or the ongoing pursuit of improvement. However, the tools available to generate the evidence needed to support those changes remain poorly matched to the task. Conventional prototyping lacks manufacturing fidelity; commercial-scale CMOs are structured around stability, not experimentation; and validated production lines cannot easily absorb the uncertainty of iterative design work.
Pilot production addresses this gap directly. By replicating critical manufacturing operations in a flexible, lower-volume environment, development teams can generate statistically meaningful data under production-representative conditions, without putting commercial supply at risk. Crucially, it is not a replacement for formal design transfer, but a means of arriving at that stage with greater confidence and fewer unknowns.
As drug delivery systems become increasingly complex, and as expectations for continuous improvement grow, such approaches are likely to play an increasingly important role. By bridging the gap between concept and commercial manufacture, pilot production enables organisations to pursue innovation with greater confidence, while maintaining the reliability and supply continuity that patients depend on.
REFERENCE
- “Medical Device Safety Communications Database”. Web Page, US FDA, accessed May 2026.

