Citation: Crowley P, Martini LG, “Optimising Drug Delivery: The Challenges and Opportunities”. ONdrugDelivery Magazine, Issue 59 (Jul 2015), pp 4-11.
By Patrick Crowley and Luigi Martini
Most medications are taken orally and provide a bolus of drug for rapid absorption. Such delivery may be satisfactory in many cases. However, absorption and distribution usually delivers drug to many tissues, organs and cells as well as to the site of activity. Such widespread presence may cause unwanted effects. Additionally, onset and duration of action may be sub-optimal.
Better information during the early stages of drug development should lead to better dosage form design and better medications. However, it has usually been impossible to generate much meaningful knowledge before efficacy and safety is established. Furthermore, not every drug is amenable to enhancement by formulation even when there is good clinical rationale for doing so.
It is important therefore to be aware of the opportunities and the limitations for designing and administering formulations that are better targeted or otherwise controlled. Current approaches, initially in oral drug delivery but also in other delivery routes, are discussed in this review. Perspectives are also presented on future possibilities for novel ways of drug delivery to optimise efficacy and reduce unwanted effects.
OPTIMISING DRUG DELIVERY/ TARGETING
The ideal medication provides the requisite amount of drug at the site of its biological action and sustains its effect for a suitable time. Requirements may be dictated by the clinical condition, the mode and dynamics of the drug’s action and patient-related considerations such as age, health, genetic makeup and presence of other clinical conditions. Drug delivery from the dosage form should ideally take account of such considerations. Historically, such dosage form design, particularly for novel structures, was constrained by lack of or limited information for optimising performance. Clinical assessment programs may have utilised dose frequencies that were based on the pharmacokinetics of the drug, with doses reflecting what was tolerated in Phase I volunteer trials. Material was usually dosed orally to optimise patient convenience and compliance. Many potentially useful materials may have failed to demonstrate safety and efficacy because of such modes of evaluation. Compound attrition was high.
“New insights concerning drug-receptor relationships, better diagnostic techniques to monitor performance, technologies for improved delivery, along with advances in molecular biology, genomics and other sciences are providing opportunities for better dosage form design and better medications…”
This situation is changing. New insights concerning drug-receptor relationships, better diagnostic techniques to monitor performance, technologies for improved delivery, along with advances in molecular biology, genomics and other sciences are providing opportunities for better dosage form design and better medications. It should lead to less attrition in novel drug development and identify possibilities for “re-inventing”(repurposing) existing drugs to improve performance in approved conditions or use in other therapeutic areas.
DRUG DELIVERY: ORAL DOSAGE
Oral dosage is likely to remain the most popular mode of drug delivery route for a number of reasons. It is important then to be aware of the factors that might impede his mode of dosage:
- It may not be possible to provide, and sustain optimum or consistent drug levels at the intended target (site of activity)
- Time of arrival at the target (and associated onset of action) may not be optimal
- Drug delivered to compartments other than site of action may evince undesirable effects.
THE GASTROINTESTINAL TRACT
A drug dosed orally can encounter several barriers, while en route to systemic compartments. It may be inactivated by low pH in the stomach or by digestive enzymes in the intestinal lumen. Designing a dosage unit to obviate such attrition may be only partially successful and confined to specific molecular constructs. Protection against pH related degradation can usually be achieved by coating with an acid-insoluble (enteric) coat. Other barriers are more difficult to surmount. Proteins and peptides are usually degraded by proteolytic enzymes in the small intestine such that there have been few successes in oral delivery of macromolecular entities. Consequently, most biopharmaceuticals are administered parenterally.
Rate of passage through the stomach and the intestinal tract may affect rate and extent of absorption. A unit, taken after food (full stomach) is likely to deliver drug later and less consistently to the small intestine, possibly delaying absorption and onset of action. The mechanism of drug action may be such that its effect can be sustained by maintaining plasma levels for longer periods than afforded by its pharmacokinetics. Hence, controlling drug release from the dosage form as the unit transits the gastrointestinal (GI) tract may prolong absorption and subsequent residence at the site of action.
Strategies for prolonging absorption include coating drug with polymeric materials, through which the drug diffuses gradually during gastrointestinal transit. Polymer coatings with pH-dependent solubility may achieve the same effect, drug being released as “pulses” in the intestinal location where polymer is soluble. However, transit rates in the small intestine, while relatively consistent are quite rapid viz 3-4 hours in healthy subjects.1 This relatively short transit time may militate against prolonging an effect if drug is rapidly eliminated and has a short duration of action. Lipidic materials such as oleic can reduce intestinal transit rate to some extent; the so-called “ileal brake” effect, but amounts required generally preclude incorporation in a conveniently-sized dosage form.2
Most drugs are absorbed from the small intestine, particularly the proximal region: absorption can be less efficient in distal parts.3
A possible strategy in such cases might involve retaining the dosage unit in the stomach, drug being gradually released and passed to the intestine, prolonging absorption and extending plasma presence. Such gastro-retention might conceptually be achieved as follows:4
- The pyloric sphincter between the stomach and intestine acts as ‘gatekeeper’, retaining larger particles in the stomach until they are suitably digested. A gastro retentive dosage form could be based on dosage unit size. Swellable polymers have been used to coat dosage forms so that unit size increases on ingestion, extending gastric residence. Drug released at a controlled rate from the retained unit sustains delivery to the intestine to prolong absorption; or
- Formulation with mucoadhesive excipients that adhere to gastric mucosa, prolonging residence, drug being released from such units at appropriate rates; or
- Systems based on so-called floating polymers, or on high density beads to provide gastro retention.
Despite such imaginative approaches, gamma scintigraphic and other studies have shown that most if not all gastro-retentive systems perform no better than large non disintegrating dosage units, taken with a meal and possibly in the evening.4
Furthermore, the gastric emptying process can be highly variable due to factors such as food (content and nature), posture (standing/prone/sleeping/sleeping orientation) and conditions such as stress, illness and age. Such unreliability could be critical, particularly with medications where consistent onset of action is important. Thus while the goal of prolonged gastric retention is a worthy one the promise remains largely unfulfilled and the strategy has attained little success as commercially viable products. There have been suggestions that drug-containing microparticles of the requisite dimensions and coated with suitable hydrophilic polymers can lodge in intestinal villi and prolong intestinal residence.5 However, there is no direct evidence to demonstrate slower intestinal transit.
PHYSICOCHEMICAL PROPERTIES OF THE DRUG
Aqueous solubility
A drug must be in solution to pass through the intestinal wall. In general terms, if solubility is less than about 1-5 mg/ml absorption might be compromised.6 However, other factors may need to be explored or considered. Material available for solubility studies, during early discovery and compound selection, may not be in the most thermodynamically stable form, or a mixture of crystalline and amorphous forms. Such materials can be more soluble than the form ultimately used, improvements to purification, isolation, crystallisation techniques providing a more thermodynamically stable but less soluble form that may be less well absorbed. Transformations to these less soluble forms are also possible during material storage or under stresses when processing.
The dynamics of precipitation and dissolution may also be important. A drug with good solubility at gastric pH might be less soluble in neutral environments but may not immediately precipitate in the intestinal milieu; absorption may not be affected. Formation of super-saturated solutions with adequate kinetic stability (solubility) may be feasible using hydrophilic polymers.7,8 There can be many exceptions to general maxims relating solubility to absorption. It is important therefore to develop good understanding of factors that contribute to and maintain supersaturation to avoid transformation to the less soluble state.
“The GI tract is replete with barriers, primed to degrade, transform or otherwise reject chemical, microbial and other harmful agents. Peptide constructs are digested by peptidases in the small intestine. This is a major barrier to oral delivery of macromolecules such as monoclonal antibodies and other protein based drugs…”
Low solubility need not necessarily result in a compound being discarded. Strategies to enhance solubility, dissolution rate and absorption include using a more soluble salt, including solubilising excipients in the dosage form, reducing drug particle size among others.9 Particle size reduction, for instance to micro- or even nano-sized particles can increase dissolution rate, aiding absorption if dissolved drug is readily removed from the drug/dissolving medium interface, allowing more drug to be dissolved. Success is not guaranteed as previously mentioned factors such as site of absorption or intestinal transit rate can also be influential. Dose of drug can also be important, a high dose requiring greater volumes of dissolving medium for solubilisation. This can complicate development programs where higher doses are tolerated and more effective than originally envisaged from preclinical studies. Dose responses may not be linear.
Permeability
Passage from the intestine to systemic compartments may involve active transport, absorption via the paracellular route or, in most cases, permeation through intestinal epithelial cells (enterocytes). Drugs best suited to this latter mode of passage are of low molecular mass and relatively lipophilic (log P = 1-3).10 It may be difficult to design molecular structures that accommodate seemingly competing requirements for good aqueous solubility for dissolution (hydrophilicity) and lipophilicity to facilitate absorption. Appropriate hydrophilic/lipophilic balance is also required for passage to organs and tissues that may be the locus of drug activity. It is difficult to design a drug molecule that is “all things to all biological sites”.
INTESTINAL ENZYMATIC BARRIERS
The GI tract is replete with barriers, primed to degrade, transform or otherwise reject chemical, microbial and other harmful agents. Peptide constructs are digested by peptidases in the small intestine. This is a major barrier to oral delivery of macromolecules such as monoclonal antibodies and other protein-based drugs. Strategies to improve protein and peptide absorption have considered enzyme inhibitors, permeation enhancers, colloidal delivery systems, nanoparticulate systems and many more. All have largely failed. Indeed the wisdom of breaching defense systems to allow peptide and protein passage has been questioned because of the possibilities for opening the route to harmful viruses and the potential for disrupting digestive and absorptive processes for dietary protein.11
Intestinal absorption can also be hindered by interactions with the glycoprotein, P-glycoprotein (P-gp) and Cytochrome P450 (CYP450) enzymes in the intestinal epithelium. These can complicate and compromise absorption. Some drugs are also inhibitors of CYP450 enzymes, preventing co-administration. Non-drug materials such as components in grapefruit juice and many herbal materials are also CYP450 inhibitors. These have been considered as formulation aids, to reduce or prevent CYP450 attrition but do not seem to have been used in dosage form design. CYP450 and P-gp enzymes also play major roles in other defence systems, being present in the liver, the blood-brain barrier and other tissues and organs.
In summary, some attractive concepts are available to facilitate or optimise oral dosage. However, variables associated with the GI tract as well as patient-associated variables such as age, lifestyle, smoking, alcohol consumption, even sleep patterns and various co-morbidities, can make oral dosage less than ideal for some drugs and some clinical conditions. Furthermore, for drugs absorbed orally the first port of call is usually the liver. This organ plays a major role in transforming materials to active moieties in the case of prodrugs, or to non-active materials for disposition. Metabolism may also occur in other tissues and organs, reducing or preventing effective drug levels reaching a specific site. Other modes of delivery or targeting may warrant consideration.
NON-ORAL, NON-INVASIVE MODES OF DRUG DELIVERY
The aforementioned vagaries of absorption and metabolic transformation can mean that only a small proportion of the drug dosed orally reaches the biological target. Moreover, drug presence in other tissues or organs can cause unwanted effects. Collateral damage of this nature has probably limited the usefulness of many compounds or arrested their progression. Prime examples concern drugs designed to be cytotoxic to cancer cells but that are also toxic to other organs, tissues or cells.
COX-2 Inhibitors are excellent anti inflammatory agents but can also cause gastric bleeding; some can also have cardiac side effects.
Parenteral administration provides a more reliable input of drug to the systemic circulation but also leads to hepatic metabolism and can “flood” the system with drug. It will not be discussed further in this review because of space constraints.
Drugs that may warrant consideration for non invasive delivery that avoids the GI tract must usually be potent as access via “less-travelled” routes is limited, these being designed to protect against ingress of harmful agents. Drug dose needs to be low. Consistency of amount delivered can also be a challenge. Nevertheless, judicious choice of drug, its form and formulation can lead to useful treatments for some clinical conditions.
INTRA-ORAL DELIVERY
Some drugs may be absorbed directly from the oral cavity. Amounts are modest so the route is generally only suited to low dose (potent) drugs. An additional, seemingly mundane but important requirement is that the drug should not be bitter-tasting or have other unacceptable organoleptic properties if used to treat chronic, non-acute clinical conditions. Otherwise, patient compliance may be compromised.
The sublingual region of the oral cavity possesses two vein complexes close to the surface that drain through facial and jugular veins, carrying drug directly to the heart and avoiding hepatic and gastrointestinal tract attrition: the route can be “drug sparing” as a consequence. Absorption is rapid and direct transport to cardiac muscle can provide prompt relief when treating conditions such as angina (glyceryl trinitrate) or pain.
| Drug | Delivery site | Indication/category | Presentation |
| Nitroglycerine | Sublingual | Angina | Tablet |
| Erythrityl | |||
| Isosorbide | |||
| Fentanyl | Analgesia | ||
| Testosterone | Buccal | Hypogonadism | Buccal path |
| Miconazole | Antifungal | Mucoadhesive tablet | |
| Verapamil | Sublingual/buccal | Antihypertensive | Chewing gum |
| Noscapine | Cough suppression | ||
| Dimenhydrinate | Motion sickness |
Figure 1: Products for intra-oral delivery
Absorption from the buccal region of the oral cavity is slower so may provide more “controlled release”. Hepatic metabolism is also avoided. Absorption can be sustained over time by formulating as bioadhesive films, possibly release controlling excipients to prolong adhesion and sustain the bioadhesive systems sublingually; buccal presence is less intrusive). Dosing can be terminated by removing the film or bioadhesive compact.
Other examples of buccal delivery systems concern chewing gums (nicotine), buccal tablets and “fast-dissolving systems” (see Figure 1).
This route is generally only suited to high potency, low dose drugs due to the limited surface area for absorption, removal of drug in swallowed saliva and the low permeability of buccal tissue. The presence of peptidases within the buccal mucosa is a also barrier to absorption of proteins as is their large molecular mass (low diffusion co-efficients). Formulation with protease/peptidase inhibitors has been considered but success, in terms of commercial products has eluded researchers to date. A comprehensive review of possibilities and challenges concerning this mode of drug delivery from Repka et al was published in 2011.12
TOPICAL DELIVERY
Topical applications may be used to treat skin bacterial and fungal infections or inflammatory conditions such as psoriasis. Product can be formulated as semi solids (creams or ointments) to prolong contact or as aerosols, foams or sprays for ease of application where skin may be sore. The formulation should be designed such that drug readily partitions from the vehicle to the outer skin layer (stratum corneum), where it may act as a reservoir for diffusion to dermal, sub dermal, possibly subcutaneous locations.
Ideally, there should be little or no systemic absorption although some might reach systemic compartments if skin is damaged, for instance. Preclinical safety studies should take account of such possibilities.
TRANSDERMAL DELIVERY SYSTEMS
Transdermal systems deliver drug through the skin to evince a systemic rather than local effect. Many transdermal medications are designed in the form of an adhesive patch, providing prolonged contact and an accurate delivery area to help dose accuracy.
As a major function of the skin is as a protective barrier there are formidable barriers to this mode of drug delivery. Rate of delivery is slow so contact with the skin needs to be prolonged and the pharmacokinetics or duration of action of the drug should be relatively long. At the same time the “continuous” (zero order) that may be associated with this mode of delivery may suit some clinical conditions or mode of drug action. Peaks and troughs may be avoided and dosing can be terminated by patch removal. It may also be feasible to provide a loading dose of drug by another route (oral/ parenteral) with concomitant or follow-up transdermal application to sustain long-term presence at the site of action. Other challenges associated with transdermal delivery can concern skin sensitisation by the drug or by penetration enhancers used in the formulation to improve absorption. Site of application can also determine rate of delivery.
| Drug | Indication | Comment |
| Clonidine | Hypertension | |
| Fentanyl | Post-operative pain | Iontophoresis (dosing can be adjusted) |
| Granisetron | Chemotherapy-induced nausea and vomiting | |
| Methylphenidate | Attention deficit disorder | |
| Nicotine | Smoking cessation | |
| Nitroglycerin | Angina | |
| Rivastigmine | Dementia | “Continuous” (zero order) delivery |
| Rotigatine | Parkinsonism/restless leg syndrome | Continuous delivery |
| Scopolamine | Motion sickness | |
| Selegline | Depression |
Figure 2: Examples of drugs formulated for transdermal delivery
Various techniques and technologies have been developed to enhance transdermal delivery. Organic solvents such as propylene glycol, incorporated in the formulation can disrupt the stratum corneum barrier and improve penetration. Iontophoresis may boost the flux of ionisable structures, a micro current device being incorporated in the application patch. Ultrasound along with “semi-invasive” modes of delivery, such as electropororation, mechanical ablation and perforation using microneedle devices have all been considered as delivery aids.13 Such innovative concepts and activities may reflect the interest in using this route as a (relatively) non-invasive mode of delivering proteins, peptides and oligonucleotides.
Microneedle-based systems are being evaluated as, for example, a means of delivering insulin for diabetes management. However, skin and subdermal layers present formidable metabolic entry barriers. These include peptidases (as well as CYP450 metabolising enzymes) in addition to diffusional barriers (molecular size) to delivery of large molecules. 14 The relatively narrow therapeutic index of insulin also requires that amounts delivered be precise. To date no insulin-based transdermal systems are available.
Figure 2 lists examples of some Transdermal medications. A number of other products are also available for hormone replacement therapy, some containing more than one drug. These are not included in the interests of brevity.
INHALATION
Alveolar and associated vascular epithelia are readily permeable, with abundant blood flow and large surface areas for absorption. Drug delivery to such tissue can be effective, particularly in treating local diseases and conditions. Onset of action can be rapid, and gastrointestinal and first-pass / first-attrition avoided. If the site of action is lung tissue there can be a “dose-sparing” effect, with reduced exposure to other sites. Well-established examples concern selective beta agonists such as salbutamol that readily relax bronchial smooth muscle: these are often used in combination with slower acting anti inflammatory agents such as glucocorticoids. Doses by inhalation are in the microgram range, rather than the mg levels required for oral administration that might have more widespread and undesirable long-term effects.
There was much concern when inhaled corticosteroids were first introduced for treating asthma but no significant unwanted effects have been manifested over several decades of use.
A major delivery challenge, whether the inhaled medication is in solid or droplet form concerns the tortuousity of the bronchial airways. If particle or droplet size is too large there are losses due to inertial impaction. Particles that are too small fail to “settle” and are exhaled. Amounts delivered to alveolar tissue may accordingly be as low as 10-20% of the inhaled dose. Clinical states such as asthma and emphysema can also affect delivery of dose. This has led to the development of sophisticated particle-generating and delivery devices, actuated by inspiration or propelled from an aerosolised container to optimise delivery attributes such as plume geometry and particle velocity, enabling more reliable, accurate and consistent dosing. An additional and important advantage with such delivery devices is capability for dose adjustment, by appropriate technology-based programming of the delivery system, providing a “personalised” dose of medication.
Other considerations for inhalation delivery include potential to elicit allergic reactions in lung tissue (drug or components such as propellants). A drug with irritant properties or which is bitter tasting is also less likely to be suitable for inhalation delivery as taste buds in the pharynx could be impacted on inspiration.
Two insulin-containing aerosol inhalation products have been approved in the US. One was withdrawn because of poor patient acceptance and suggestions, unproven, that it was associated with lung cancer risks due to deposition of insulin on lung tissue. A second product, Mannkind’s Affrezza, was launched recently but long-term sales data is not available at the time of writing. Judgement on non-invasive delivery of insulin has accordingly to be deferred at this time.
INTRANASAL DELIVERY
Advantages associated with intranasal delivery concern high permeability of nasal epithelia for hydrophobic drugs, an extensive underlying vascular bed, avoidance of “first-pass” hepatic metabolism and of gastro intestinal attrition.
The susceptibility of biopharmaceutical products to degradation when dosed via the GI tract, along with their increasing prominence as medicinal agents has spurred much interest in non-invasive routes for delivering these to systemic compartments. The intranasal route is no exception. However, permeation of polar drugs and macromolecular entities like proteins and peptides is low.15 Furthermore, the nasal airways are designed to protect pulmonary tissue from hazardous materials and to hinder systemic absorption. Aerodynamic behaviours and anatomical features of the nasal regions, with the majority of droplets deposited in the anterior nasal mucosa due to inertial impaction and sedimentation present significant barriers to efficient delivery. Ciliary motion and a protective mucous layer designed to intercept particles, micro-organisms and other unwanted materials are additional hurdles.16 The nasal cavities can be highly sensitive to the presence of irritants; sneezing in response to a stimulus can expel a medication. The enzymatic barriers in the nasal epithelium are also similar to those hindering other modes of systemic entry: CYP450 enzymes are present at even higher levels than in liver. Peptidases and proteases are also present.17
Reliable and efficient delivery of protein- based biopharmaceuticals by this route may be as challenging as for other non invasive modes of dosage. So-called absorption enhancers have been evaluated as a means of increasing amounts of drug that are absorbed. These present their own challenges. Bioadhesives to prolong contact may also cause mucosal damage if used chronically.
Vaccines can be administered intranasally as there is potential for inducing superior antibody response in the upper respiratory tract.18 They may be formulated as a spray mist containing mucoadhesive polymers, adhesion to the nasal mucosa improving immune response.19 Available space prevents discussion of other modes of non-invasive delivery such as rectal, ocular, vaginal, and colonic delivery.
FUTURE PERSPECTIVES
The locus of activity for many medicines may be within a specific organ or cell type and precise targeting by molecular design may not be feasible. In such cases drug delivery strategies warrant consideration. Two topics are considered here, namely delivery to the brain and intracellular targeting to illustrate delivery concepts being considered. These should be viewed as illustrative as they do not represent the extent of activities in the area. Many other innovative approaches are also being explored.
DELIVERY TO THE BRAIN
Anxiety, Depression, neurodegenerative conditions such as Alzheimer’s and Parkinsonism, eating disorders, drug addiction and other clinical conditions are considered to be brain-associated.20,21 Neurodegenerative conditions in particular respond poorly to current medications. This has serious sociological and societal implications for future healthcare. Dementia-related conditions increase exponentially with age; almost 40% of people aged 75-84 or older in the US are estimated as suffering from Alzheimer’s disease.
Total healthcare spending on geriatric healthcare currently consumes approximately 16% of US GDP, 75% being spent on treating chronic illnesses. Longer lifespans are likely to inflate such numbers. Trends in many other countries are probably similar. Societal burdens could become immense.
The less-than-stellar records of many current medications may be due inadequate levels of drug reaching the site of activity. The blood-brain barrier (BBB) presents formidable hurdles to passage of many agents, particularly those that are polar in nature. It has been estimated that more than 98% of current drugs do not surmount this hurdle to any significant extent.23
The BBB is more readily crossed by nonpolar (lipophilic) entities but these are likely to be poorly absorbed from the GI due to their low solubility, or are metabolised in hepatic and other locations to polar structures for ready elimination. Consequently, drug discovery programs have focused to some extent on providing water-soluble drugs. Plasma protein binding also militates against brain delivery.
Drugs administered by the oral route and others already discussed in this paper are invariably transported via the bloodstream (lymph in some instances). They encounter the BBB so passage to the brain is limited. Molecular design may help lower the barrier but higher doses may be required so that sufficient passes to the brain. This may lead to “drug overload” and side effects in other organs and tissues throughout the body. Consequently there is much interest in strategies for better-targeted brain delivery.

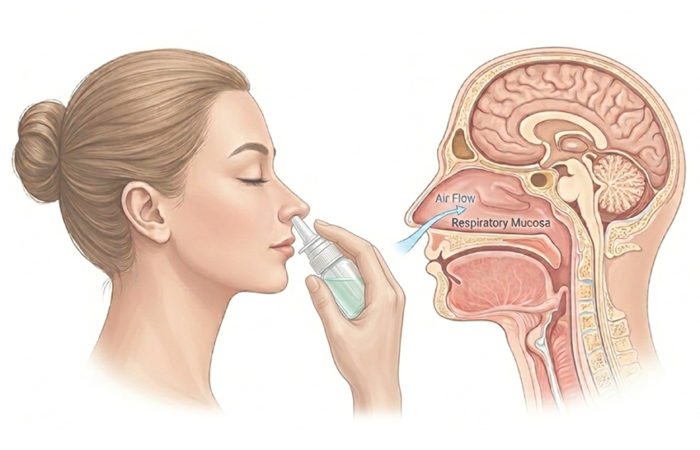
Figure 3: Nose-to brain delivery. (Adapted from original image sourced with permission from Boundless Learning).
One possibility, meriting consideration concerns passage from the upper nasal cavity via trigeminal and olfactory pathways, thereby avoiding the BBB.20,24 Aromatherapy, based on using volatile oils and other aromatic compounds as mood-altering agents is based on such concepts. Vapours rapidly reach the brain and a much lower dose than delivered conventionally might provide effective therapy if drug could be delivered as vapour.
Figure 3 provides a schematic for disposition and fate of drug administered intranasally. A fraction may be eliminated by degradation or mucociliary clearance, more may be absorbed through the anterior nasal mucosa, or by swallowing. Absorbed materials encounter and are largely recycled (rejected) at the BBB. A fraction may reach the upper nasal region and, if in suitable form, some may enter the brain via the olfactory and trigeminal conduits.
Thus, mucociliary clearance, enzymatic degradation, swallowing, possibly other modes of disposition are likely to reduce amounts reaching the upper nasal cavity. Furthermore, drug in solution or particulate form may not be in a suitable state to enter the olfactory/trigeminal pathways are unlikely to facilitate passage of liquids or solids (the usual way to effect delivery). These are structured to allow passage of vapours. Ideally, potentially useful drugs for delivery by the nose-to-brain route would be in the vapour state but few drugs are likely to have been designed with such properties in mind. Crystalline solids of good purity are usually favoured in drug discovery and development, ideally in soluble form for acceptable oral absorption.
“Ideally, potentially useful drugs for delivery by the nose-to-brain route would be in the vapour state but few drugs are likely to have been designed with such properties in mind. Crystalline solids of good purity are usually favoured in drug discovery and development, ideally in soluble form for acceptable oral absorption…”
There is evidence that brain pathology associated with conditions such as Alzheimer’s disease, depression and Parkinsonism may be related to chronic inflammatory processes. It has also become evident that the nonsteroidal anti-inflammatory agents, COX-2 Inhibitors appear to be beneficial in such conditions.21,25,26 However, small pilot trials with NSAIDs dosed orally, while providing encouraging results with Alzheimer’s patients, were compromised by high dropout rate due to GI side effects.27,28
Other trials provided similarly confounding results. It would seem that the GI and other side effects of NSAID’s dosed orally would constrain their use for treating or preventing such chronic conditions. However, better targeted delivery to the brain via the upper nasal cavity could avoid widespread disposition in other tissues, require much lower dosage and have a significantly better side effect profile.
The NSAID ibuprofen, and possibly other NSAID’s, reportedly exhibit vapour pressure.29,30,31 Evidence of volatility of other drugs is somewhat lacking but few existing drugs would have been intentionally designed to be volatile. It is possible, however, that other well-established drugs could be isolated in volatile form; free base or acid rather than salt for instance.
There may be scope for innovative chemistry to provide material in a volatile form that retains its molecular integrity. Functional requirements for so-called odorants have been defined in terms of vapour pressure, polarity, lipophilicity and surface activity.32 Such definitions might provide useful templates for molecular design, or searches for existing agents.
Other possibilities for facilitating brain entry via olfactory/trigeminal routes might utilise solutions of drug in propellants of the kind currently used for lung delivery of anti-asthma medications. The rapid vaporisation of such propellants might leave drug in vapour form for sufficiently long for passage to the brain to occur.
The extracellular-transport-nature of delivery as vapour via the upper nasal region might also facilitate rapid onset of drug action, a major benefit in brain-related conditions such as migraine or seizures. It is difficult however to conceive that macromolecular entities might be delivered in this way. Molecular mass considerations suggest that they would be unlikely to be volatile. However, claims have been made that the interferon, IFN beta -1b bypasses the BBB, being delivered preferentially to the brain via the olfactory/trigeminal route, albeit in rats.33 No reports could be found on successful delivery in humans despite the ten-year gap to this publication. Interest remains high however.
INTRACELLULAR DELIVERY
The locus for activity of many drugs is likely to be intracellular. However, many protective systems impede cell entry very effectively. Drug constructs are being designed to overcome such barriers using strategies to capitalise on modes of cell recognition and transport, and many others. Much such activity (and innovative approaches) concern oncology drugs, solid tumours in particular being resistant to entry. At the same time the cytotoxic nature of many anticancer agents is such that the ideal drug or medication should be noncytotoxic to non-cancer cells and tissues but be activated, within the cancerous tissue or cells.

Figure 4: Hinged DNA nanobot which forms a cage to contain drug molecules. It can exist in the a) open and b) closed configurations. Reproduced with permission from the Wyss Institute.34
Nano robots (“nanobots”) have been conceived and designed with such requirements in mind, being assembled from DNA strands. DNA nanobots, in addition to being “biocompatible” also have valuable “design capability”, a long single strand of DNA being capable of coupling with shorter strands to provide a suitably “sized and shaped DNA cage” to accommodate a drug. “DNA hinges” in such clam-shell-like constructs provide capability to exist in open or closed form (see Figure 4a & 4b). The closed shell, in conjunction with anchor strands within the cage and complimentary DNA linker strands attached to the drug, secure drug retention. The cage is locked by DNA double helices.34
The external surface of the nanobot is designed to recognise and dock only to cancer cells. On cell entry by the nanobot, a cancer specific protein within the cell “unlocks the cage” to release drug in a “trojan horse-like” manner. Such constructs have been shown in vitro to target a series of six different cancer cell lines: cage-containing antibody fragments consistently induced cell apoptosis.34 Such imaginative delivery concepts might conceivably serve as “platform technologies” for intracellular targeting of other therapeutic agents.
Many other innovative approaches, too numerous to reference here, are being propounded and tested for better-targeted drug delivery. Some will ultimately be successfully trialled in clinical programs and become part of the armamentarium of medical scientists in treating illness and disease.
“This review has accordingly focused on the limitations as well as the possibilities for dosage-form design so that informed choices can be considered in oral formulation programs…”
CONCLUSIONS
Systems that are currently available to target or modify the delivery of drug have advantages and limitations that can be associated with the clinical condition, the patient or the molecular biology/mode of action and physical characteristics of the specific drug. There is no “one size fits all”.
This review has accordingly focused on the limitations as well as the possibilities for dosage-form design so that informed choices can be considered in oral formulation programs. There is also much interest and associated activity in concepts that may provide more precise and localised drug delivery to render such materials more effective and safer. Such insights, along with better diagnostic concepts and technologies can greatly help in assessing the utility of novel constructs as drugs or in improving the performance of those already being used.
REFERENCES
- Davis SS, Hardy JG, Fara JW, “Transit of pharmaceutical dosage forms through the small intestine”. Gut, 1986, Vol 27, pp 866-892.
- Dobson CL, Davis SS, Chauhan S, Sparrow RA, Wilding IR, “The effect of oleic acid on the human ileal brake and its implications for small intestinal transit of tablet formulations”. Pharm Res, 1999, Vol 16(1), pp 92-96.
- Barr et al, “Differential Absorption of amoxicillin from the human small and large intestines”. Clin Pharmacol & Therapeutics, 1994, Vol 56(3), pp 279-285.
- Coffin MD, Burke MD, in Ch 17, “Controlled Release in Oral Drug Delivery”. Springer/CRS Publications.
- Autant P, Selles JP, Soula G, “Medicinal and nutritional microcapsules for oral administration”. US Patent 6022562 (2000).
- Florence AT, Attwood D, “Physicochemical Principles ofPharmacy” p21: Macmillan, 3rd Ed, London (1998).
- Brouwers J, Brewster ME, Augustijns P, “Supersaturating drug delivery systems: The answer to solubility-limited oral bioavailability?” J Pharm Sci, 2009, Vol 98(8), pp 2549-2572.
- Curatolo W, Nightingale JA, Herbig SM, “Utility of Hydroxypropylmethylcellulose Acetate Succinate (HPMCAS) for Initiation and Maintenance of Drug Supersaturation in the GI Milieu”. Pharm Res, 2009, Vol 26, pp 1419- 1431.
- Crowley PJ, Martin LG, “Physicochemical Approaches to Enhancing Oral Absorption”. Pharm Tech Eur, 2004, Vol 16(9), pp 18-27.
- Singh BN, “Drug Delivery: Oral Route”. Encycl Pharm Sci Tech, 4th Ed, 2013, pp 1122-1149. Taylor & Francis, New York, NY, US.
- Shah RB, Ahsan F, Khan MA, “Oral delivery of proteins: Progress and prognostications”. Crit Rev Ther Drug Carrier Systems, 2002, Vol 19, pp 135-169.
- Repka MA, Chen L-l, Chan RS, “Controlled Release in Oral Drug Delivery (CRS 2011)”. Springer Publications Chapter 16, Buccal Drug Delivery.
- Brown MB, Martin GP, Jones SA, Akomeah FK, “Dermal & Transdermal Drug Delivery Systems: Current &Future Prospects”. Drug Del, 2006, Vol 13 (3), pp 175-187.
- Banja AK, “Transdermal & Intradermal Delivery of Therapeutic Agents: Application of Physical Technologies”. CRC Press.
- Illum L, “Nasal Drug Delivery – possibilities, problems and solutions”. J Control Release, 2003, Vol 87, pp 187-198.
- Djupesland PG, “Nasal Drug Delivery Devices; characteristics and performance in a clinical perspective – a review”. Drug Del Translat Res, 2013, Vol 3, pp 42-62.
- Sarkar MA, “Drug Metabolism in the Nasal Mucosa”. Pharm Res, 1992, Vol 1, pp 1-9.
- Rudin A, Riise GG, Holmgren J, “Antibody responses in the lower respiratory tract and male urogenital tract in humans after nasal and oral vaccination with cholera toxin B subunit”. Infect Immun, 1999, Vol 67, pp 2884-2890.
- Hagenaars N, Mania M de JP et al, “Role of trimethylated chitosan(TMC) in nasal residence time, local distribution and toxicity of an intranasal influenza vaccine”. J Control Release, 2010, Vol 144, pp 17-24.
- Chapman CD et al, “Intransal Treatment of Central Nervous System Dysfunction in Humans”. Pharm Res, 2013, Vol 30, pp 2475-2484.
- Köhler O, et al, “Effect of Antiinflammatory Treatment on Depression, Depressive Symptoms, and Adverse Effects, A Systematic Review and Meta-analysis of Randomized Clinical Trials”. JAMA Psychiatry, 2014, Vol 71(12), pp 1381-139.
- Herbert LE, Weuve J, Scherr PA, Evans DA, “Alzheimer’s Disease in the US (2010-2050 estimated using the 2010 Census”. Neurology, 2013, Vol 80(19), pp 1778-83.
- Gomez D, et al, “Intranasal treatment of neurodegenerative diseases and stroke”. Frontiers in Biosci, 2012, S4, pp 74-89
- Johnson NJ, Hanson LH, Frey WH, “Trigeminal Pathways Deliver a Low Molecular Weight Drug from the Nose to the Brain and Orofacial Structures”. Mol Pharmaceut, 2010, Vol 7(3), pp 884-893.
- Practico D, Trojanowski JQ, “Inflammatory Hypotheses: novel mechanisms of Alzheimer’s neurodegeneration and new therapeutic targets”. Neurobiol Aging, 1997, pp 441-445.
- Bartels AL, Leenders KL, “Cyclooxygenase and neoroinflammation in Parkinson’s Disease Neurodegeneration”. Current Neuropharmacol, 2010, Vol 8, pp 62-68.
- In t’ Veld BA et al, “Nonsteroidal anti-inflammatory drugs and the risk of Alzheimer’s disease”. N Engl J Med, 2001, Vol 345(21), pp 1515-21.
- Rogers J et al, “Clinical Trial of indomethacin in Alzheimer’s Disease”. Neurol, 2005, Vol 43, pp 1609-1611.
- Perlovich GL, Kurkov SV, Hansen LKR, Bauer-Brandel, “A Thermodynamics of Sublimation, Crystal lattice Energies and Crystal Structures of Racemates and Enantiomers of Ibuprofen”. J Pharm Sci, 2004, Vol 93(3), pp 564-666.
- Kurkov SV, Perlovich GL, “Thermodynamic studies of Fenbufen, Diflusinal and Flurbiprofen: Sublimation, solution and solvation of biphenyl substituted drugs”. Int J Pharmaceut, 2008, Vol 357, pp 100- 107.
- Ertel KD, Heasley RA, Chakrabarti A, Carstensen JT, “Determination of Ibuprofen Vapour Pressure at Temperatures of Pharmaceutical Interest”. J Pharm Sci, 1990, Vol 79(6), pp 23-31.
- Leffingwell & Associates, “Olfaction”. (www.leffingwell.com/olfaction.htm).
- Ross TM et al, “Intranasal administration of interferon beta bypasses the blood-brain barrier to target the central nervous system and cervical lymph nodes: a non-invasive treatment strategy for multiple sclerosis”. J Neuroimmunol, 2004, Vol 151(1-2), pp 66-77. 34. http://wyss.harvard.edu.
Previous article
WHAT DO CUSTOMERS NEED IN ORAL DOSE DEVELOPMENT?Next article
MIR IMRAN, RANI THERAPEUTICS