

To Issue 186
Citation: Bedford T, “LVSC Delivery: How Volume and Concentration Requirements are Reshaping Device Selection”, ONdrugDelivery, Issue 186 (May 2026), pp 45–49.
Tony Bedford considers how the rise in biologic formulations together with a strong shift towards subcutaneous administration is shaping the drug delivery industry, particularly in relation to large-volume subcutaneous delivery.
In previous ONdrugDelivery articles (2020–2021), Phillips Medisize has explored the wearable drug delivery market and how on-body injector (OBI) devices were struggling to break through in the < 5 mL market. These articles explored the “identity crisis” of such devices, with multiple descriptors and acronyms, the rise in biologic formulations and the potential for wearables delivering greater than 5 mL – with oncology and the trend towards switching from intravenous (IV) to subcutaneous (SC) delivery as possible drivers.
Fast forward to 2026, and it is now increasingly evident that the growth in biologics, combined with a strong drive towards SC administration, is pushing the industry towards a much wider range of delivery volumes and, consequently, the potential for a broader set of device options.
THE RISE OF SC FORMULATIONS
It is now 20 years since Abbott’s (now AbbVie)1 Humira®2 (adalimumab) and Amgen/Immunex’s Enbrel®3 (etanercept) were first approved in autoinjectors, both of which achieved substantial market success with these devices.
Compared with IV infusion administered in hospital or clinic settings, the advantages of an SC route of administration (RoA) are well established. For patients, this includes greater tolerability and increased convenience, with reduced treatment times (minimal preparation, drug administration in seconds) and no need for time-consuming in-patient visits. Increasingly, the drug can be self-administered at a time and place that suit the patient.
From a healthcare industry perspective, this reduces burden, with fewer patients requiring healthcare professional (HCP) administration or infusion chair occupancy. For pharmaceutical companies, SC delivery can provide a means of patent life extension and differentiation, with benefits extending to HCPs and patients by providing greater convenience. This is reflected in the fact that, of the top 10 best-selling proprietary drug products by sales revenue, eight are approved and available in SC form, with the remaining two approved in oral RoA, as shown in Table 1.
| Drug Name | Owner(s) | Therapeutic Area | 2025 Sales* | Approved With SC Form? |
| KEYTRUDA® | Merck | Cancer | $31.7B | Yes |
| MOUNJARO® | Lilly | Diabetes | $22.9B | Yes |
| OZEMPIC® | Novo Nordisk | Diabetes | $19.9B | Yes |
| DUPIXENT® | Sanofi/Regeneron | Autoimmune | $17.8B | Yes |
| SKYRIZI® | AbbVie | Autoimmune | $17.5B | Yes |
| ELIQUIS® | Bristol Myers Squibb/Pfizer | Cardiovascular | $14.4B | No |
| DARZALEX® | Johnson & Johnson | Cancer | $14.3B | Yes |
| BIKTARVY® | Gilead | HIV | $14.3B | No |
| ZEPBOUND® | Lilly | Obesity | $13.5B | Yes |
| WEGOVY® | Novo Nordisk | Obesity | $12.4B | Yes |
* All figures from respective owners’ full year reported financial results.
Table 1: Top ten drug products by 2025 sales revenue.
To illustrate the rise of SC delivery further, as of 2024, approximately half of all approved and clinical proprietary injectables were formulated this way.4
WHAT THIS MEANS FOR LVSC DELIVERY
Many SC drug agents can readily be self-administered using established formats such as autoinjectors, prefilled syringes (PFSs) or pen injectors, largely because their delivery volumes are in the sub-2 mL range, and the advantages of these devices are well documented.
Since 2012, many large-volume subcutaneous (LVSC) drugs, defined here as those administered subcutaneously with volumes > 2 mL, have been approved. This includes a small number of anti-cancer agents that originated or switched from IV to SC administration.
In terms of delivery, these products generally fit into one of four categories:
- Multiple Bolus Injections: Depending on the volume required, the full dose may be delivered via two or more injections using autoinjectors or PFSs. Typically, this means each injection is limited to no more than ~2 mL. Studies have explored the suitability of using autoinjectors for large-volume injection.5
- Bolus “Push” Injection Enabled by Hyaluronidase6: This approach refers to larger-volume injections, typically delivered from a syringe and administered by an HCP in a clinical setting. An example is Johnson & Johnson’s DARZALEX FASPRO (daratumumab and hyaluronidase-fihj), delivered as a 15 mL bolus over three to five minutes. Several drugs of this type contain the permeation enhancer hyaluronidase, facilitating faster and more convenient SC delivery of larger volumes. Table 2 shows approved cancer agents in SC form, demonstrating the prevalence of hyaluronidase.
- OBI: A patch-pump device with an integrated needle, worn directly attached to the body. Devices may be electromechanical or mechanically powered. Currently approved devices require some level of user loading or filling but are suited for self-administration.
- Near-Body Injector (NBI): An ambulatory pump with a tethered cannula or infusion set. These devices may be electromechanical or mechanically powered and can deliver injections or infusions at controlled rates appropriate to the application.
| Drug Name | Typical SC Volume |
| VELCADE® (bortezomib) | Circa 2 mL (more than one injection can be administered) |
| HERCEPTIN HYLECTA™ (trastuzumab and hyaluronidase-oysk) |
5 mL |
| RITUXAN HYCELA® (rituximab/hyaluronidase human) |
11.7 mL/13.4 mL |
| PHESGO® (pertuzumab/trastuzumab/hyaluronidase-zzxf) |
10 mL/15 mL |
| DARZALEX FASPRO® (daratumumab and hyaluronidase-fihj) |
15 mL |
| TECVAYLI® (teclistamab-cqyv) | < 2 mL per injection (more than one injection can be administered) |
| TALVEY® (talquetamab-tgvs) | < 2 mL per injection (more than one injection can be administered) |
| OPDIVO® QVANTIG (nivolumab and hyaluronidase-nvhy) |
5 mL/7.5 mL/10 mL |
| RYBREVANT® (amivantamab-vmjw) | < 29 mL |
| KEYTRUDA QLEX™ (pembrolizumab and berahyaluronidase alfa-pmph) |
2.4 mL/4.8 mL |
Table 2: LVSC cancer agents.
Research by Green et al shows that a considerable percentage of injectables are in SC form, with a number anticipated to be developed as LVSCs, in many cases with increasing drug concentrations.4 This trend is expected to continue in the coming years.
CHALLENGES FOR THE DEVICE INDUSTRY
This LVSC pipeline trend presents several challenges for the device industry, particularly the need to deliver injections across a wide range of volume tiers, as illustrated in Figure 1. The largest “segment” falls within the 2–5 mL volume range.
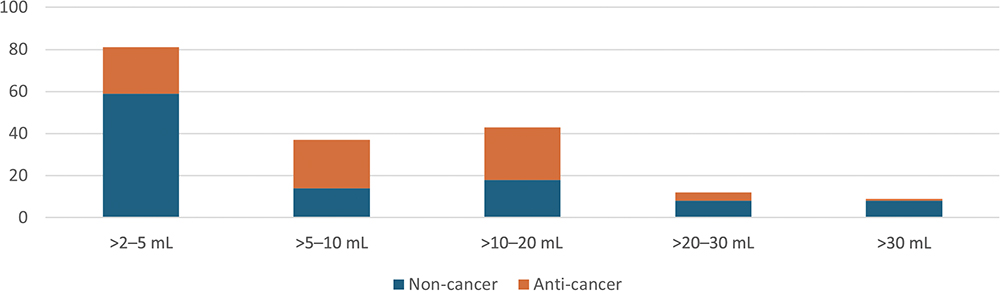
Figure 1: Volume requirements of potential LVSCs.4
Besides injection volume, evolving delivery technology must also address additional needs, including:
- Drugs for chronic self-injection
- HCP administration in a range of settings
- Delivery of biologics, which may involve challenging characteristics such as greater viscosity or cold-chain considerations
- A shift towards less frequent dosing.
Anecdotally, prefilled solutions using proven primary containers are preferred, although user-filled or user-loaded devices offer an acceptable alternative.
DEVICE OPTIONS ARE DIVERSE
An examination of approved and emerging LVSC devices shows a wide range of configurations, with no single solution clearly dominating, as shown in Table 3.
| Prefilled & pre-loaded |
Prefilled, user-loaded |
User-filled | Integrated needle | Tethered cannula | Mechanical | Electro-mechanical | |
| Handheld; Vial and Syringe |
✓ | ✓ | ✓ | ||||
| Autoinjector/PFS | ✓ | ✓ | ✓ | ✓ | |||
| OBI | |||||||
| NBI | ✓ | ✓ | ✓ | ✓ | ✓ |
![]()
Table 3: Potential device configurations for LVSC.
“FROM A TECHNOLOGY PERSPECTIVE, THE FOCUS OF DEVELOPMENT IS ON BALANCING INJECTION SPEED, FORMULATION COMPLEXITY AND USABILITY, BUT THE MATHS STILL NEEDS TO ADD UP.”
LVSC devices in development are largely focused on devices capable of delivery volumes between 5 and 50 mL, although the lower end of this range may remain within reach of large-volume autoinjectors (or PFSs), particularly where the economics of multiple autoinjectors/PFSs (or even a single syringe and manual push) are competitive. In these instances, the drug is transferred from vial to syringe for manual bolus push, although a small number of cancer centres have adopted near-body syringe pumps.7 Roche’s PHESGO (pertuzumab trastuzumab/hyaluronidase-zzxf) 10 mL injection (maintenance dose) is approved in the EU for administration outside of clinical settings.8 From a technology perspective, the focus of development is on balancing injection speed, formulation complexity and usability, but the maths still needs to add up.
A PREDICTION FOR DEVICES
The diversity of needs and technologies suggests that a range of device solutions will be necessary to support the growing LVSC market.
Based on current trends, it is reasonable to expect that over the next few years the LVSC pipeline will continue to grow, with some high-dose drugs being developed exclusively for SC administration, bypassing the IV route altogether. LVSC biosimilars may also emerge, further expanding the market. Additional permeation enhancers beyond hyaluronidase are anticipated to become available, complementing the market success of Halozyme’s (San Diego, CA, US) ENHANZE® and increasing the ease with which larger volumes can be delivered subcutaneously, with Alteogen’s (Daejeon, South Korea) berahyaluronidase being approved in Merck’s (Darmstadt, Germany) KEYTRUDA QLEX9 (pembrolizumab).
What might this mean for LVSC delivery technology? Continued emphasis on self-administration is likely, focusing on convenience for the patient and HCP, away from hospital settings. A recent approval of note is Johnson & Johnson’s DARZALEX becoming the first oncological injectable approved for administration by patients or caregivers in Europe and delivered directly from a PFS.10
Near-body injection devices have recently been rolling out globally, with examples including the continuous infusion of Parkinson’s drugs (for example, AbbVie’s Vyalev™ (foscarbidopa and foslevodopa) pump and for frequent injection of myasthenia gravis and SC immunoglobulin drugs (for example, KORU’s FreedomEDGE™).11
Such devices offer performance characteristics resembling traditional syringe pumps but in a more compact, ambulatory form, and could be considered for the replacement of manual push currently employed in cancer care. At the same time, mechanically powered OBIs could represent a significant breakthrough for LVSC devices and cancer care alike. Indeed, the Sanofi (Paris, France) Sarclisa® (isatuximab-irfc) cancer drug has been recommended for EU approval by the Committee for Medicinal Products for Human Use using Enable Injections‘ EnFuse® OBI.12
Market acceptance of larger-volume handheld devices remains uncertain. Autoinjectors in the 5 mL range are well advanced in development (for example, Ypsomed’s YpsoMate® 5.5 and SHL Medical’s Maggie® 5.0), while manual self-administered PFSs are already approved and marketed (Argenx (Amsterdam, Netherlands) VYVGART Hytrulo® (efgartigimod alfa and hyaluronidase-qvfc)).13
If uptake of large-volume autoinjectors is limited, the market may open further for OBIs in the > 5 mL space, perhaps with lower volumes continuing to be addressed by multiple bolus injections (for example, with more than one autoinjector). Two OBIs with injection volumes of ≥ 10 mL have already been approved with others in development, including the BD Libertas™, which is currently undergoing clinical trials.14 Conversely, large-volume autoinjectors such as Halozyme’s HVAI™, an autoinjector developed for up to 10 mL formulations containing ENHANZE, could disrupt this trajectory.
In the near term, whether or not we see more of these devices reach the market, wider adoption of syringes and manual push may continue, although this is unlikely to represent an optimal outcome for the patient or end users. Figure 2 summarises these predictions across delivery modalities and volume ranges.
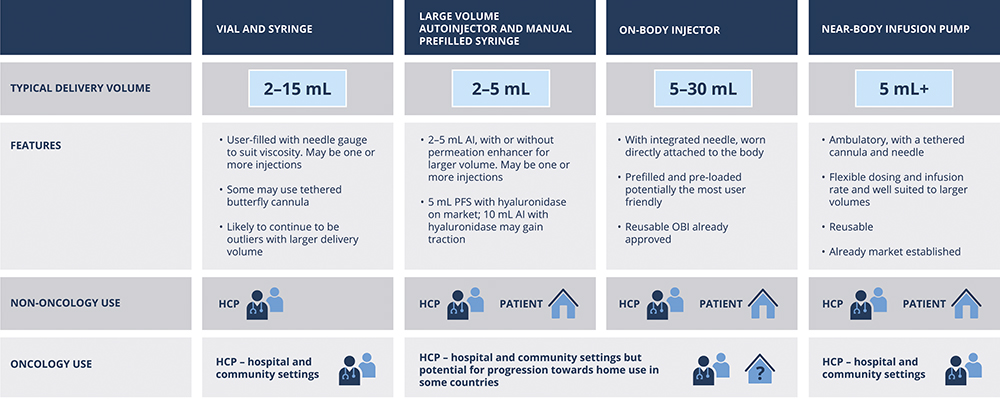
Figure 2: Predictions for LVSC delivery technology.
“INCREASINGLY, IT APPEARS THAT THE INDUSTRY IS AT THE BEGINNING OF AN IMPORTANT AND DYNAMIC PERIOD FOR LVSC DRUG DELIVERY.”
Increasingly, it appears that the industry is at the beginning of an important and dynamic period for LVSC drug delivery. For pharmaceutical teams, this reinforces the importance of making device and delivery decisions early, in parallel with formulation strategy, balanced against the uncertainties that high-concentration formulation can bring during earlier stages of development.
ACKNOWLEDGEMENTS
The author wishes to acknowledge and thank Phil Green, President of Chesapeake Pharma LLC, for his research and knowledge of the LVSC space. Since co-authoring a research paper published in 2024,4 he is widely recognised for his expertise in this field.
All trademarks and registrations are the property of their respective owners.
REFERENCES
- “Abbott drugs business to be called AbbVie on split”. Reuters, Mar 21, 2012.
- “Abbott Laboratories Receives FDA Approval For New HUMIRA(R) Delivery Device”. BioSpace, Jun 26, 2006.
- Agrawal A, “FDA Approves Enbrel Autoinjector”. HealthDay, Jun 22, 2006.
- Green P, Schneider A, Lange J, “Navigating large-volume subcutaneous injections of biopharmaceuticals: a systematic review of clinical pipelines and approved products”. Mabs, 2024, Vol 16 (1), art 2402713.
- Schneider A et al, “Autoinjectors for large-volume subcutaneous drug delivery: a review of current research and future directions”. Expert Opin Drug Deliv, 2023, Vol 20(6), pp 815–830.
- Kang D et al, “Dispersive effects and focused biodistribution of recombinant human hyaluronidase PH20: A locally acting and transiently active permeation enhancer”. PLoS One, 2021 Vol 16(7), art e0254765.
- Ammor W et al, “5PSQ-151 Optimisation of the subcutaneous administration of daratumumab”. Eur J Hosp Pharm, 2022, Vol 29 (1), art A165.
- “CHMP recommends EU label update for Roche’s Phesgo to allow administration outside of clinical settings”. Press Release, Roche, Apr 30, 2025.
- “FDA approves KEYTRUDA QLEX™ (pembrolizumab and berahyaluronidase alfa-pmph) injection for subcutaneous use in adults across most solid tumor indications for KEYTRUDA® (pembrolizumab)”. Press Release, Merck & Co, Sep 19, 2025.
- “Johnson & Johnson’s DARZALEX® (daratumumab) becomes the first oncology injectable approved for administration by patients or caregivers”. Press Release, Johnson & Johnson, Mar 27, 2026.
- “KORU Medical Systems Receives FDA 510(k) Clearance for Delivery of RYSTIGGO® (rozanolixizumab-noli), Expanding Label for FreedomEDGE® Infusion System”. Press Release, KORU, Jan 29, 2026.
- “Press Release: Sanofi’s Sarclisa subcutaneous formulation administered via on-body injector recommended for EU approval by the CHMP to treat multiple myeloma”. Press Release, Sanofi, Mar 27, 2026.
- “argenx Announces FDA Approval of VYVGART Hytrulo Prefilled Syringe for Self-Injection in Generalized Myasthenia Gravis and Chronic Inflammatory Demyelinating Polyneuropathy”. Press Release, argenx, Apr 10, 2025.
- “BD Announces First Pharma-Sponsored Clinical Trial Using BD Libertas™ Wearable Injector Technology for Biologic Drugs”. Press Release, BD, Jul 23, 2015.