Citation: Scimgeour I, “Medical Training Devices in the Home”. ONdrugDelivery Magazine, Issue 52 (Sep 2014), pp 42-45.
As home-managed disease states, medical devices and user groups diversify and proliferate helping ever more people, Ian Scrimgeour explores the growing role of the trainer device, and shows how the right trainer can greatly help reduce adverse events, improve adherence and build user satisfaction and confidence.
“Especially for kinaesthetic learners, training devices are increasingly being used. These trainer devices are non-functional, containing no drug or needle and are ideally configured to feel the same as the real device…”
INTRODUCTION
Progress in modern medicine and device design increasingly means we are able to monitor, manage and treat our ailments at home. As discussed in the October 2013 Association for the Advancement of Medical Instrumentation (AAMI) summit on Healthcare in Nonclinical Settings (Herdon, VA, US), this is a laudable trend. Moving treatment out of the clinical environment has many advantages1 but places greater emphasis on the patient or carer to use drugs and devices as intended. As home-treatable disease states, devices and their users diversify, ensuring effective and safe device deployment is an increasingly complex challenge for the industry. Device design must consider these diverse user groups and always, training plays a vital role. How can training methodologies advance to ensure each user has the opportunity to learn, becoming comfortable and confident with the safe use of their device? The value of the training device is becoming increasingly apparent.
ADVANCING HEALTHCARE AT HOME
With current and projected growth in home healthcare, increasing numbers of chronic and acute medical conditions are being managed in the domestic non-clinical environment. In the US, it is estimated between 8.6 and 12 million people currently receive home healthcare, increasing to 27 million in 2050.10 Advances in technology and medical care systems are enabling this shift, lowering the cost of healthcare whilst improving patient quality of life and independence.2 This trend is global as technology advances and populations grow.
As the medical devices driving this paradigm shift devolve and diversify, home device user groups and disease states become similarly diverse. Where once home-use medical devices were restricted to a select group of indications and patient groups, they are now used for an ever expanding range of treatments and conditions. Adding further complication, devices used in the home are subjected to significantly different environments and user profiles than in the more controlled environment of hospitals, surgeries and clinics. As extolled in usability engineering standards,3 robust user-centred design identifies user groups and provides device designs that attempt to understand and accommodate the users, their habits, expectations and capabilities. A device’s risk profile is anticipated during development and monitored through the products lifecycle. However, sometimes such diverse user abilities and expectations pose hazards which seem difficult to resolve in the device design alone. A good risk assessment can identify issues which can leave development teams head-scratching for solutions, such as the following:
- Users can have an established mental model of use based on a similar or drastically different device, creating unanticipated expectations and actions.
- A user may not be capable of absorbing all information from the training session provided
- A user’s anxiety can impede their ability to follow seemingly simple usage steps. Emotion can overwhelm cognitive reasoning.4
TRAINING IS ESSENTIAL
No matter how effective the device design, training is an essential element in overcoming risks like those just described and, as such, fulfils a fundamental role in the application of modern medicine. There are many reported cases where adverse events are attributed to poor training. For example, a retrospective review of adverse events associated with adolescent use of insulin pumps identified poor education (device training) as the cause in 47 out of 102 cases, the majority of which led to hospitalisation.5
Currently the medical device, pharmaceutical and healthcare industries use the following training methods to impart learning to the user or patient:
- Written Instructions for Use (IFU) – a regulatory bare minimum, often augmented with:
- Visual stimuli, diagrams and pictures – pictorial representation of what to do
- Video instructions – via DVD, website or mobile app
- Instructor-led learning – a healthcare professional (HCP), such as a nurse or other clinician, who introduces the device and method of use
- Peer learning – a fellow patient provides a demonstration or guidance on device use.
There is another training tool available to industry: training devices.
Training devices are growing in popularity as a way of enhancing learning and mitigating use error issues. To explore how these support medical device use we need to consider the different ways through which one might learn.
LEARNING STYLES
Different people have different learning styles, as summarised in Fleming’s well-known VARK model of learning which divides learners into four categories of learning preference.6
- Visual learners (looking at images and pictures)
- Auditory learners (hearing instruction)
- Reading-writing preference learners (reading instruction)
- Kinaesthetic learners or tactile learners. (doing and practising).
BOX 1: TEN BENEFITS OF HOME-USE TRAINING DEVICES
- Promotes kinaesthetic learning through practice and experience
- Promotes repetition at home leading to enhanced learning
- Reduces anxiety. Giving the user a chance to get used to the device and activity promotes the alleviation of concerns. Especially important prior to the first “real” device use
- Improves compliance. Not being comfortable with a medical device and being unsure as to how to use it effectively can have a significant impact on patient compliance
- Prevents waste of high-value drugs – non-adherence costs US$100-300 billion (£62-£185 billion) each year 8
- Provides additional risk mitigation for risk analysis e.g. failure modes and effects analysis (FMEA)
- Creates competitive advantages – users look favourably at pharmaceutical companies which they perceive to care enough to provide trainer devices
- Mitigates curtailed or missed introductory training sessions. Current training is often less than that mandated by the drug company. They may recommend 30 minutes training, but in reality healthcare providers sometimes don’t have that time with patients.
- Prevents “training erosion” where information is diluted or changed when passed on, for example, from device company to drug company, to distributor, to healthcare provider, to patient. A training device allows the device company direct contact with the user.
- It allows device training to take place in the correct usage environment and promotes private learning, for example, in the bedroom at home, not the consultation room at the health clinic. Training at home in private allows the user to explore the device and usage experience.
“What should a training device be? There are two methodologies available: deploying the precise replication of the parent device experience or deploying a multi-sensory enhanced educational device…”
Mixed learning styles are often utilised to maximise learning during the initial introduction to a new medical device. Pharmaceutical companies, hospitals, clinics or support groups often provide a HCP led instructional session for the new patient. During such a session the patient is able to hear from the HCP, read the training material, look at charts and photographs and observe a device like the one they will be using. By such methods visual, auditory and reading learners are given means to learn. To support learning further, especially for kinaesthetic learners, training devices are increasingly being used. These trainer devices are non-functional, containing no drug or needle and are ideally configured to feel the same as the real device so the patient can role play device use.
Medical device companies will construct training materials and requirements and the patient is presented with visual, auditory, written and tactile information. However, what happens to the patient’s knowledge after their initial introductory consultation?
LEARNING RETENTION
Using mixed learning styles in the initial consultation, the patient is given all the information they require to understand the correct use of the device. Of course once the patient has left the consultation room, the reality is quite different and full learning is usually not achieved for the following reasons:
- Insufficient time available. Time for training session is often reduced or eroded. The HCP will often have other pressures on their time and a 30-minute training session may be cancelled or reduced.
- Information overload. Being introduced to a new medical device is often a very emotional, abstract or alien experience for the patient, all of which can increase patient stress significantly and inhibit learning.
- Learning degradation. Learned knowledge degrades rapidly over time. A patient can leave an instructional session feeling confident that have absorbed adequate knowledge, but without reinforcement the knowledge will degrade, as described first by Ebbinghaus.7
Figure 1 is a representation the Ebbinghaus forgetting curve, describing how information degradation is diminished with repeated repetition and practice. At each time point, the learner practices and reviews device use, resulting in improved long-term retention.

Figure 1: Representation of Ebbinghaus forgetting curve, knowledge degradation chart.
In summary:
- Knowledge can be better retained if it is reinforced repeatedly after the initial introduction.
- Multi-style learning promotes better retention.
- Kinaesthetic learning is a valuable but often overlooked learning style.
A way to leverage these three key learning mechanisms is by providing training devices that users can take home. In Box 1 we identify ten benefits of home-use training devices.
ASSIGNING VALUE TO TRAINING DEVICES
Investing in a training device can provide significant added value to both device company and user. When done smartly the development and manufacturing costs can be a fraction of the parent device cost and, whilst assigning monetary value to some of the softer benefits outlined above can be challenging, the cost of non-adherence is well documented. This is especially true of the more expensive drugs and treatments currently being prescribed. If the confidence and knowledge provided by a training device prevents users missing their $1,000 dose of medicine, then the return on investment can occur very rapidly.
TRAINING DEVICE STRATEGY
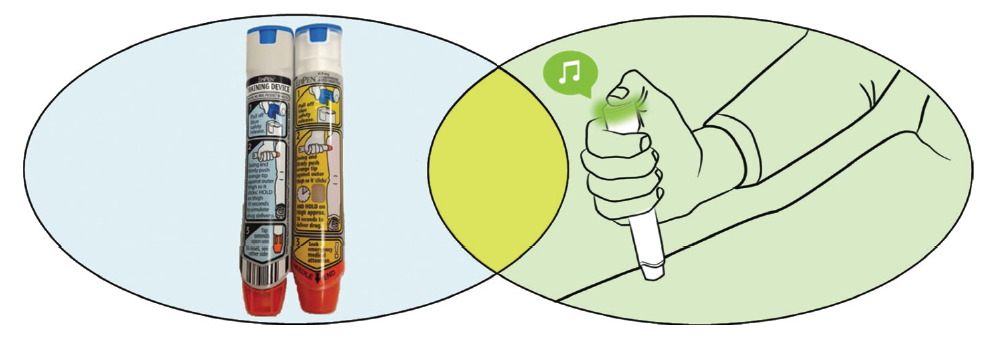
So what should a training device be? There are two methodologies available: deploying the precise replication of the parent device experience or deploying a multi-sensory enhanced educational device (Figure 2).

Figure 2: Replication and enhanced educational training device options.
A replication device seeks to match the parent device user experience as precisely as possible. For example, a complex force profile from the parent device shall be engineered into the trainer device ensuring the user has the opportunity to run through the precise tactile experience.
Alternatively, a multi-sensory enhanced educational device does not rely on precise replication (though replication to some extent plays a part), rather audio, visual and tactile enhancements guide the user through the usage experience. These give clear positive reinforcement for the correct actions and correspondingly highlight incorrect actions.
These options are not mutually exclusive and a hybrid solution may be the most effective. Selecting the preferred option or combination of options depends on issues such as parent device complexity, the nature of anticipated failure modes and the projected training device complexity and cost.
The SelfDose® from Janssen / West Pharmaceutical Services (shown in Figure 3) is a single-use injection device intended for user groups with reduced dexterity, for example the aging population.9 Based around a 1 ml prefilled syringe, it’s ergonomically designed and allows the user to control injection speed, as quickly or slowly as they like, which also means it is suitable for a variety drug and biologics over a wide range of viscosities. A training device was created to enable the users to overcome anxiety and become familiar with the tactile response felt during a real injection. It accurately recreates the progressive resistance felt by the user during an injection without having any needle or drug product, it feels just like the real thing, allowing multiple “dryruns” before using the real device.

Figure 3: West’s SelfDose® device, for which a replication training device was created.
TRAINING DEVICE DEVELOPMENT
Training device development can be initiated at any point during the parent device development programme, it’s never too late, though of course earlier is better. In itself a non-intrusive training device with no sharps, active drug ingredient or diagnostic capability is not a medical device, which means that a full GMP or 13485 programme may not be required and a more rapid development programme is possible, providing it fits with and supports the parent device development and regulatory requirements. Careful consideration needs to be given to the impact on the use of the parent device of course, and care needs to be taken not to create additional failure modes. (For example, it is crucial to avoid the scenario where the trainer device is confused with the real device at times of need.)
In order for medical device companies to achieve the rapid and flexible development required, often third-party developers can help. A training device development team studying the parent device development, function and modes of use, can provide rapid, clearly resolved training device solutions. Using partners with sound basis in medical device development, engineering and usability will help the training device development programme effectively and efficiently create the training device to suit.
CONCLUSION
As home-use medical devices come to the fore, training devices provide means to educate and train diverse and complex user groups, by allowing them the chance to roleplay, practice and prepare at home. In providing such training devices, medical and pharmaceutical companies can improve learning, improve adherence and reduce patient/user anxiety. Together this creates a more robust home-use medical device proposition, which should smooth the regulatory approval route and ultimately reduce adverse events.
REFERENCES
- “A Vision for Anywhere, Everywhere Healthcare”. AAMI Report, 2014, pp 6-8. (Available at: http://www.aami.org/publications/summits/HomeHealthcare.pdf)
- “Medical Device Home Use Initiative”. US FDA Report, April 2010.
- ISO/TC 210. IEC 62366:2007.
- Norman DA, “Emotional Design”. Basic Books, 2004. (ISBN-10: 0-465- 05135-9).
- Cope JU, Morrison AE, Samuels- Reid J. “Adolescent Use of Insulin and Patient-Controlled Analgesia Pump Technology: a Ten-Year FDA Retrospective Study of Adverse Events”. Pediatrics, 2008, Vol 121.
- Leite WL, Svinicki M, Shi Y, “Attempted Validation of the Scores of the VARK: Learning Styles Inventory With Multitrait, Multimethod Confirmatory Factor Analysis Models”. Educational & Psychological Measurement, 2009, Vol 70, pp 232-229.
- Ebbinghaus H, “Memory: a Contribution to Experimental Psychology”. [trans.] Henry A. Ruger and Clara E. Bussenius. 1885.
- Koreoneos G, “Adherence Through Education”. Pharmaceutical Executive, August 2010.
- Krulevitch P, “Human Factors Testing and Design Evolution of a New Self-Injection Device”. Proc. IBC’s Human Factors for Drug- Device Combination Products Conference, 2014 (Philadelphia, PA, US).
- Wan H, et al, “Current Population Reports”. Census Bureau, 2005. pp. 23-209.
SelfDose® is a registered trademark of West Pharmaceutical Services, Inc, in the US and other jurisdictions.