

To Issue 186
Citation: Desai M, Hageman M, Chen W, “Antibody-Drug Conjugates: An Emerging Frontier in IV to SC Conversion”, ONdrugDelivery, Issue 186 (May 2026), pp 63–69.
Dr Mehul Desai, Dr Michael Hageman and Dr Wei Chen examine the growing antibody-drug conjugate market, the unique formulation challenges these therapies present for subcutaneous delivery and how innovations in on-body injector technology may offer a practical path forwards.
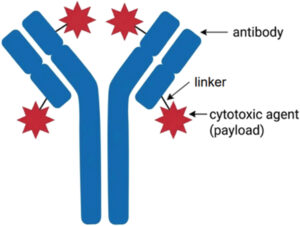
Figure 1: ADC components – the location of the payload can vary based on the molecule.
THE ADC LANDSCAPE: A DRUG CLASS COMING OF AGE
Before exploring the formulation challenges that antibody drug conjugates (ADCs) present for subcutaneous (SC) delivery, it is important to understand their history, structure and mechanism of action. At their core, ADCs are engineered molecules that combine the specificity of a monoclonal antibody with the cell-killing potency of a cytotoxic small-molecule payload. As shown in Figure 1, ADCs have three components: the antibody, the linker and the payload (usually a cytotoxic agent). The antibody component targets a specific antigen expressed on the surface of tumour cells, while the payload, connected via a chemical linker, is released once the ADC is internalised, delivering the cytotoxic agent directly to the cancer cell.1 A simplification of this process is depicted in Figure 2.
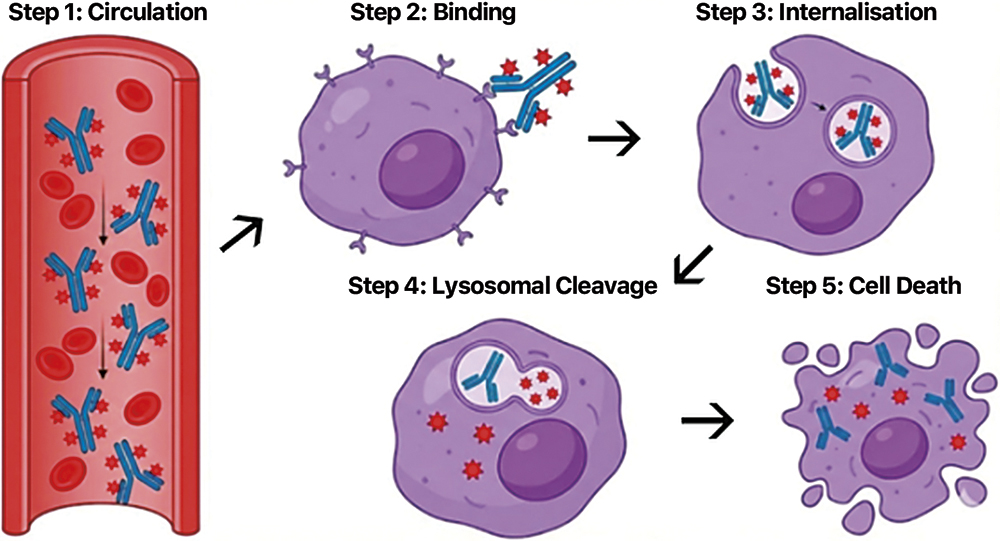
Figure 2: Simplified ADC process.
“THIS TARGETED APPROACH OFFERS A CLEAR THERAPEUTIC ADVANTAGE: IT CONCENTRATES THE CHEMOTHERAPY AT THE TUMOUR SITE WHILE MINIMISING SYSTEMIC EXPOSURE, WHICH CAN REDUCE THE SIDE EFFECTS TYPICALLY ASSOCIATED WITH CONVENTIONAL CHEMOTHERAPY APPROACHES.”
This targeted approach offers a clear therapeutic advantage: it concentrates the chemotherapy at the tumour site while minimising systemic exposure, which can reduce the side effects typically associated with conventional chemotherapy approaches. This concept has translated into meaningful clinical outcomes and the ADC market is rapidly growing as a result. Estimates suggest that the value of this drug class will grow from approximately US$15 billion (£11 billion) in 2025 to $20 billion in 2026. By 2031, it is projected to reach $71 billion, which reflects a compound annual growth rate of nearly 29% between 2026 and 2031.2 More than 15 ADCs have received US FDA approval and over 400 are currently in clinical development globally to treat a wide range of autoimmune diseases and cancers.3,4
A critical parameter for understanding the delivery of ADCs is the drug-to-antibody ratio (DAR), which refers to the average number of cytotoxic payload molecules conjugated to each antibody. To help visualise what the DAR means with regards to the molecular structure, Figure 3 shows a simplified comparison of three different DAR levels. The DAR is one of the most important variables of an ADC, influencing its efficacy and formulation behaviour. Higher DAR values increase the amount of cytotoxic drug delivered per antibody molecule, which can enhance anti-tumour activity. However, a higher DAR also increases hydrophobicity, which can accelerate aggregation, reduce stability and complicate formulation development.5
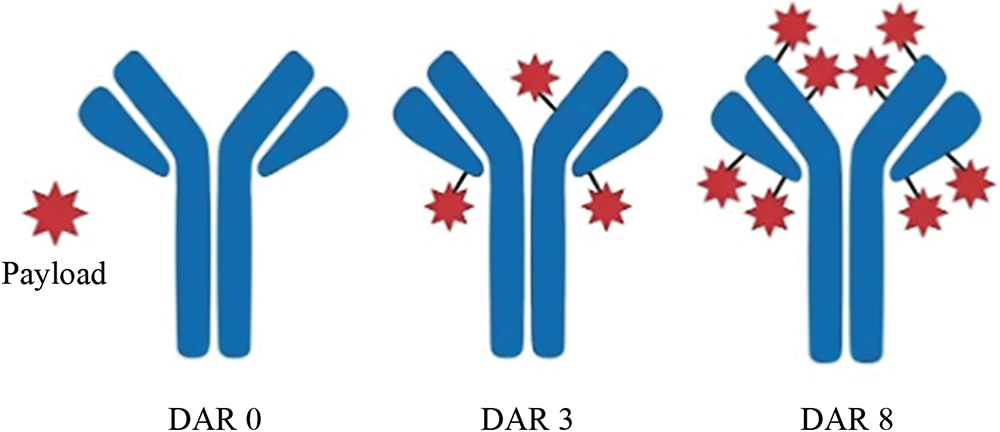
Figure 3: Visualisation of DAR levels.
The DAR also has specific implications for SC delivery. When an ADC is injected subcutaneously, it forms a depot in the tissue that is gradually absorbed into systemic circulation. During this dwell time, skin proteases, including cathepsin B, can cleave the linker and release the cytotoxic payload locally.6 Essentially, this would be Step 4 in Figure 2 occurring prematurely within the SC layer. A DAR 8 ADC, such as trastuzumab deruxtecan or sacituzumab govitecan, carries four times more payload per molecule than a DAR 2 ADC, meaning the local exposure to free cytotoxic drug at the injection site is proportionally greater. This makes linker stability in the SC environment a key consideration for the ADC delivery strategy. Many approved ADC payloads are hydrophobic and prone to aggregation at higher concentrations, while newer payloads like DXd have been engineered for reduced hydrophobicity.
As shown in Table 1, a notable feature shared by all but one FDA-approved ADC is lyophilisation. This is not coincidental. ADC linkers, particularly peptide-based linkers, are highly sensitive to temperature and shear forces, making them susceptible to premature cleavage in liquid formulations. Lyophilisation removes water from the product, creating a more stable environment that minimises these degradation pathways.9 While lyophilisation solves the stability problem, it introduces its own downstream challenges for drug delivery.
| ADC | Target | DAR | Payload | Linker Type | Formulation | Route |
| Gemtuzumab ozogamicin | CD33 | ~2.5 | Calicheamicin | Cleavable | Lyophilised | IV |
| Brentuximab vedotin | CD30 | ~4 | MMAE | Cleavable | Lyophilised | IV |
| Ado-trastuzumab emtansine | HER2 | ~3.5 | DM1 | Non-cleavable | Lyophilised | IV |
| Inotuzumab ozogamicin | CD22 | ~6 | Calicheamicin | Cleavable | Lyophilised | IV |
| Polatuzumab vedotin | CD79b | ~3.5 | MMAE | Cleavable | Lyophilised | IV |
| Enfortumab vedotin | Nectin-4 | ~3.8 | MMAE | Cleavable | Lyophilised | IV |
| Trastuzumab deruxtecan | HER2 | ~7.8 | DXd (topoisomerase I inhibitor) |
Cleavable | Lyophilised | IV |
| Sacituzumab govitecan | Trop-2 | ~7.6 | SN-38 (topoisomerase I inhibitor) |
Cleavable | Lyophilised | IV |
| Loncastuximab tesirine | CD19 | ~2.3 | SG3199 (PBD dimer) | Cleavable | Lyophilised | IV |
| Tisotumab vedotin | Tissue Factor | ~4 | MMAE | Cleavable | Lyophilised | IV |
| Mirvetuximab soravtansine | FRα | ~3.5 | DM4 (maytansinoid) | Cleavable | Liquid | IV |
| Datopotamab deruxtecan | Trop-2 | ~4 | DXd (topoisomerase I inhibitor) |
Cleavable | Lyophilised | IV |
| Telisotuzumab vedotin | c-Met | ~3.1 | MMAE | Cleavable | Lyophilised | IV |
Table 1: Commercially available FDA-approved ADCs and key characteristics.3,4,7,8 All FDA approved ADCs are administered intravenously and all but one are formulated as lyophilised powders for reconstitution.
WHY ADCs ARE STRONG CANDIDATES FOR SC CONVERSION
The broader trend of converting intravenous (IV) biologics to SC formulations has been well established over the past decade. Monoclonal antibodies for oncology have successfully transitioned to SC delivery, driven by shorter administration times, reduced healthcare resource use and patient preference. ADCs, despite their additional complexity, share several characteristics that make them attractive candidates for SC conversion.
“EARLIER LINE USE MEANS LONGER TREATMENT DURATION AND A GREATER TOTAL NUMBER OF INFUSIONS OVER THE COURSE OF THE THERAPY.”
First, ADCs are increasingly being used in earlier lines of therapy. Trastuzumab deruxtecan has moved into frontline HER2-positive breast cancer, enfortumab vedotin is now approved in frontline urothelial carcinoma (in combination with pembrolizumab) and multiple ADCs are being studied in frontline settings across solid tumours. Earlier line use means longer treatment duration and a greater total number of infusions over the course of the therapy. Each IV infusion requires clinic chair time, nursing resources and patient and caregiver travel. The cumulative burden on both patients and healthcare systems is already substantial and continues to grow.
Second, the pharmacokinetic (PK) profile of SC delivery may offer advantages for ADCs. SC administration inherently produces a lower Cmax and a more gradual absorption profile compared with IV delivery. Exposure-response analyses of trastuzumab deruxtecan across 639 patients demonstrated that different ADC toxicities are driven by different PK metrics – grade ≥3 interstitial lung disease was associated with peak intact ADC concentrations (Cmax), while haematologic toxicities such as neutropenia and thrombocytopenia were driven by average free payload concentrations over time.10 Whether the lower Cmax profile associated with SC delivery could favourably influence specific ADC toxicities remains to be established clinically, but the pharmacological rationale warrants investigation.
Third, for a growing number of patients, the ADC may be the only IV therapy in their regimen. Several ADCs are used as monotherapies and combination partners are increasingly becoming available as SC formulations. With the recent approval of SC pembrolizumab, a combination such as enfortumab vedotin plus pembrolizumab could theoretically be delivered entirely without IV access if the ADC component were available as an SC formulation.11 For these patients, converting the ADC to SC delivery could eliminate the need for infusion chair time altogether, potentially enabling administration outside of a traditional infusion suite.
CHALLENGES OF TRANSITIONING ADCs TO SC DELIVERY
Despite the compelling rationale, transitioning ADCs from IV to SC delivery presents formulation and delivery challenges that go beyond those encountered with conventional monoclonal antibodies. These challenges have contributed to a limited, and somewhat troubled, history of SC ADC development.
Linker stability in SC tissue
The SC space contains numerous protease enzymes, including cathepsin B, which is known to cleave the peptide-based linkers used in many ADCs.12 When a linker is cleaved prematurely at the injection site, the cytotoxic payload is released locally rather than at the tumour. For certain ADCs, this has manifested as erythema and tissue necrosis at injection sites in preclinical models.13,14 While newer linker technology may offer improved stability, comprehensive characterisation of linker behaviour in the SC compartment remains limited.
“ALMOST ALL FDA-APPROVED ADCs ARE LYOPHILISED. THIS REQUIRES RECONSTITUTION WITH A DILUENT BEFORE ADMINISTRATION, ADDING PREPARATION STEPS, TIME AND THE POTENTIAL FOR HUMAN ERROR.”
Lyophilised formulations
As noted earlier, almost all FDA-approved ADCs are lyophilised. This requires reconstitution with a diluent before administration, adding preparation steps, time and the potential for human error. Lyophilised products are difficult to deliver with traditional SC delivery devices, such as autoinjectors and prefilled syringes, due to the fact that these devices are primarily designed for ready-to-use liquid formulations. Reconstitution at the point of care is feasible in clinical settings but adds complexity for at-home infusion.
Volume requirements
ADC doses are often weight-based and, when reconstituted at current IV concentrations, can result in volumes ranging from approximately 5 mL to well over 20 mL depending on the specific ADC and patient weight. This far exceeds the capacity of conventional SC delivery devices such as autoinjectors and presents significant challenges for manual syringe delivery.15,16 Concentrating ADC formulations to reduce volume is particularly difficult because the linked cytotoxic payloads are inherently hydrophobic, which drives aggregation and increased viscosity at higher concentrations far more readily than with normal antibodies. Developing a high-concentration liquid SC formulation of a molecule that cannot be stored as a lower-concentration liquid for IV use represents a formidable, and in many cases impractical, development challenge.17
What the Preclinical Data Show and Do Not Show
In February 2026, preclinical data were presented demonstrating hyaluronidase co-formulation with two approved ADCs, both with DAR ~8, identified as ADC 1 and ADC 2. The data, generated in a Yucatan minipig model with three animals per SC group and a single IV control animal, showed reduced injection site ADC retention with hyaluronidase co-formulation versus SC alone (87% reduction for ADC 1, 51% for ADC 2 at 24 hours) and a lower serum Cmax with SC versus IV administration (75% lower for ADC 1, 61% lower for ADC 2).18
Despite injection site tolerability being the central challenge for SC delivery of ADCs, no formal safety endpoints were included in the study design. No histopathology scoring, inflammation markers or macroscopic injection site observations were described. While these data represent an encouraging signal for the broader SC delivery opportunity of ADCs, several limitations warrant careful consideration.
The IV control group consisted of a single animal (N=1), limiting the reliability of any cross-route PK comparison, while the SC groups included only three animals each. The study was single-dose only and did not report bioavailability despite equivalent doses being administered across all groups. However, PK modelling projected that a higher SC dose would be needed to achieve equivalent systemic exposure to IV, implying that SC bioavailability was meaningfully lower. This higher dose was modelled but never tested, meaning the tolerability conclusion is based on a potentially sub-therapeutic dose level.
Most critically, the study did not measure linker stability within the SC tissue. For ADCs, linker integrity in the extracellular environment is a critical variable in determining suitability for SC delivery, as premature cleavage releases the cytotoxic payload into healthy tissue rather than within the target tumour cell. It was acknowledged that free payload measurements may have been overestimated due to linker instability during sample processing and analysis, further underscoring the limitations of the available data in addressing this fundamental question.
Importantly, the Cmax reduction demonstrated in this study is a fundamental property of the SC route of administration itself, not unique to hyaluronidase co-formulation. The SC-alone groups (without hyaluronidase) also showed substantially lower Cmax compared with IV, which is an expected and well-understood consequence of slower absorption from SC tissue. Any SC delivery method, whether administered via syringe, pump or on-body injector (OBI), would be expected to produce a similar reduction in Cmax relative to IV. This inherent benefit of SC delivery should not be conflated with that of hyaluronidase.
What this data does demonstrate is that the hyaluronidase co-formulation has faster clearance of intact ADC from the injection site – supported by the tissue PK data – with meaningful reductions in local ADC retention at 24 hours compared with SC alone.
However, the metric of greatest clinical relevance for ADC safety is not how quickly the intact molecule clears but how much free cytotoxic payload is released locally. On this measure, the presented data show no meaningful differentiation between SC only and SC with hyaluronidase. Free payload concentrations in both the serum and skin tissue tracked closely between the two groups, with overlapping variability at all measured timepoints. If both SC delivery approaches produced comparable free payload profiles and if local tolerability was reported as acceptable in both groups, this raises a fundamental question: is hyaluronidase co-formulation necessary at all for SC delivery of ADCs?
This question has practical implications. OBIs, pumps and syringes can deliver the same large volumes subcutaneously without requiring reformulation of the drug product. For ADCs, which are universally formulated as lyophilised powders requiring reconstitution, avoiding the additional complexity of co-formulating with a permeation enhancer represents a meaningful reduction in time, cost and risk.
OBIs: A Device-Centric Approach
OBIs offer an alternative approach to large-volume SC delivery that does not require co-formulation with a permeation enhancer, although they are compatible with them. This preserves existing formulation integrity and avoids the complexity of adding a second biologic excipient. Crucially, the larger volume capacity of OBIs removes the pressure to formulate a high-concentration format, allowing the ADC to remain in a more stable, lower-viscosity solution.
Published data indicate that the tissue surface area exposed to an injected drug is primarily a function of injection volume rather than flow rate.19 However, the lower, more consistent tissue pressures generated by elastomeric delivery, compared with tissue pressure characteristics associated with rapid bolus injection, may reduce local tissue disruption and the associated inflammatory response, which is relevant for ADCs given that inflammation can upregulate protease activity at the injection site.20,21 While this hypothesis has not been directly tested with ADCs, the mechanistic rationale is consistent with the goal of preserving linker integrity during SC transit.
Clinical evidence supporting OBI technology for large-volume SC oncology delivery continues to build. In the Phase 3 IRAKLIA trial, which evaluated isatuximab delivered via an OBI versus IV in patients with relapsed/refractory multiple myeloma, infusion reactions occurred in only 1.5% of OBI injections, compared with a 25% infusion reaction incidence with IV administration – a near 17-fold reduction.22 Notably, 99.9% of OBI injections were completed without interruption. Preference for the OBI over manual syringe push has been demonstrated for physicians, pharmacists, nurses and, most importantly, patients.15,16, 22–24
Addressing the Lyophilisation Challenge
As all approved ADCs are lyophilised, any SC delivery solution must address the reconstitution step. Published literature has identified the reconstitution step as the largest source of error among patients self-administering lyophilised drugs, with confusion around the number of steps and supplies contributing to deviations and sterility breaches.25 Integrating reconstitution into a device workflow would reduce this complexity.
Several approaches to automated or semi-automated reconstitution are emerging across the drug delivery landscape. Dual-chamber syringes and cartridges separate the lyophilised drug and diluent within a single container, allowing mixing at the point of use without manual transfer steps. However, these systems require the drug manufacturer to reformulate and repackage the product into a new primary container, which adds development time, regulatory complexity and cost.
An alternative approach uses a dual-vial design in which the original drug product vial and a separate diluent vial are both loaded into the delivery device simultaneously (Figure 4). The system reconstitutes and transfers the drug product, while preserving the original container closure system. For ADCs, where all approved products are manufactured and stored in vials, this approach avoids the need for new primary container development and maintains the validated stability profile of the existing formulation. This may be particularly relevant for enabling at-home administration of lyophilised, large-volume SC biologics, where simplifying the reconstitution process is essential for safe, reliable use outside of clinical settings.

Figure 4: An approach to simplifying reconstitution of ADCs.
“THE TRANSITION OF ADCs FROM IV TO SC DELIVERY IS NOT A QUESTION OF IF, BUT WHEN AND HOW. THE MARKET DRIVERS ARE CLEAR: A RAPIDLY GROWING DRUG CLASS, INCREASING USE IN EARLIER TREATMENT LINES, A STRONG PATIENT AND PROVIDER PREFERENCE FOR SC ADMINISTRATION AND A GLOBAL HEALTHCARE SYSTEM UNDER MOUNTING CAPACITY PRESSURE.”
LOOKING AHEAD
The transition of ADCs from IV to SC delivery is not a question of if, but when and how. The market drivers are clear: a rapidly growing drug class, increasing use in earlier treatment lines, a strong patient and provider preference for SC administration and a global healthcare system under mounting capacity pressure. The formulation and delivery challenges are real but addressable with current large-volume SC technologies, each offering distinct paths forwards.
For ADCs in particular, the choice of SC delivery strategy deserves careful evaluation beyond simple PK matching. The unique features of ADCs, specifically the presence of cytotoxic payloads connected by protease-sensitive linkers, the reliance on lyophilised formulations and the potential for local tissue toxicity, introduce considerations that are absent from conventional monoclonal antibody IV-to-SC conversions. A device-centric approach that preserves the existing formulation, uses the original container closure system, delivers at a low pressure and accommodates lyophilised products would be particularly well suited to this drug class.
As the ADC pipeline continues to expand, drug manufacturers will increasingly need to evaluate SC delivery options early in their development programmes. The ability to convert directly from an IV vial-based formulation to SC delivery, with minimal reformulation, container closure changes or co-formulation with exogenous enzymes, represents a significant practical advantage that could accelerate time to market and reduce development risk.26,27
REFERENCES
- Drago JZ, Modi S, Chandarlapaty S, “Unlocking the potential of antibody-drug conjugates for cancer therapy”. Nat Rev Clin Oncol, 2021, Vol 18(6), pp 327–344.
- “Antibody drug conjugates market size & share analysis – growth trends and forecast (2026-2031)”. Report, Mordor Intelligence, Feb 2026.
- “21 approved ADCs worldwide: the ultimate guide (Updated 2025)”. Web Page, Huateng Pharma, accessed Mar 2026.
- Wang R et al, “Antibody-drug conjugates (ADCs): current and future biopharmaceuticals”. J Hematol Oncol, 2025, Vol 18(1), art 51.
- Junutula JR et al, “Site-specific conjugation of a cytotoxic drug to an antibody improves the therapeutic index”. Nat Biotechnol, 2008, Vol 26(8), pp 925–932.
- Varkhede N, Bommana R, Schöneich C, Forrest ML, “Proteolysis and oxidation of therapeutic proteins after intradermal or subcutaneous administration”. J Pharm Sci, 2020, Vol 109(1), pp 191–205.
- “ADC linker technology overview”. Web Page, Biochempeg, accessed Mar 2026.
- “Review and formulation analysis of 14 antibody-drug conjugates (ADCs) approved by FDA up to 2022”. Web Page, BOC Sciences, accessed Mar 2026.
- Cho E et al, “Stability of antibody drug conjugate formulations evaluated using solid-state hydrogen-deuterium exchange mass spectrometry”. J Pharm Sci, 2021, Vol 110(6), pp 2379–2385.
- Okamoto H et al, “Exposure-response relationships in patients with HER2-positive metastatic breast cancer and other solid tumors treated with trastuzumab deruxtecan”. Clin Pharmacol Ther, 2021, 110(4), pp 986–996.
- “FDA approves enfortumab vedotin-ejfv with pembrolizumab for locally advanced or metastatic urothelial cancer”. Web Page, FDA, accessed Mar 2026.
- Lyon RP et al, “Reducing hydrophobicity of homogeneous antibody-drug conjugates improves pharmacokinetics and therapeutic index”. Nat Biotechnol, 2015, Vol 33(7), pp 733–735.
- Yaseen AA, Rahman MA, Tumey LN, “Subcutaneous administration of antibody-drug conjugates”. Curr Pharmacol Rep, 2026, Vol 12, art 1.
- Bodyak ND et al, “The dolaflexin-based antibody-drug conjugate XMT-1536 targets the solid tumor lineage antigen SLC34A2/NaPi2b”. Mol Cancer Ther, 2021, Vol 20(5), pp 896–905.
- Desai M et al, “Evaluating nurse preferences for a novel on-body delivery system vs. manual syringes for large-volume subcutaneous drug administration: a survey study”. Drug Deliv, 2025, Vol 32(1), art 2484278.
- Sánchez Avello N et al, “Subcutaneous administration of isatuximab in patients with multiple myeloma by an on-body delivery system: results of a nurse survey”. Front Oncol, 2025, Vol 15, art 1547108.
- Hobson AD et al, “Optimization of drug-linker to enable long-term storage of antibody-drug conjugate for subcutaneous dosing”. J Med Chem, 2023, Vol 66(13), pp 9161–9173.
- Halozyme Therapeutics, “Q4 2025 earnings call presentation”. Presentation, Feb 2026.
- Kim T et al, “Ex vivo tissue provides insight into bleb dynamics during large-volume subcutaneous injection”. Pharm Res, 2026, Vol 43(2), pp 483–493.
- Yan D, Wang HW, Bowman RL, Joyce JA, “STAT3 and STAT6 signaling pathways synergize to promote cathepsin secretion from macrophages via IRE1alpha activation”. Cell Rep, 2016, Vol 16, pp 2914–2927.
- Zamolodchikova TS, Tolpygo SM, Svirshchevskaya EV, “Cathepsin G – not only inflammation: the immune protease can regulate normal physiological processes”. Front Immunol, 2020, Vol 11, art 411.
- Ailawadhi S et al, “Isatuximab subcutaneous by on-body injector versus isatuximab intravenous plus pomalidomide and dexamethasone in relapsed/refractory multiple myeloma: Phase III IRAKLIA study”. J Clin Oncol, 2025, Vol 43(22), pp 2527–2537.
- Desai M et al, “Evaluating pharmacist preferences: preparation of a novel on-body delivery system vs. high-resistance, manual syringes for large-volume subcutaneous drugs”. J Oncol Pharm Pract, 2025.
- Loughran C et al, “Pharmacist and nurse preferences for preparing large-volume subcutaneous oncology drugs during a patient capacity crisis in the United Kingdom: a discrete-choice study comparing manual syringe vs. an on-body injector”. Poster, HOPA Annual Conference, 2026.
- Franzese C, Aulton ME, Auffret T, “The burden of at-home preparation of lyophilized parenteral medications”. Expert Opin Drug Deliv, 2019, Vol 16(3), pp 187–198.
- Desai M et al, “Insights from a survey of drug formulation experts: challenges and preferences in high-concentration subcutaneous biologic drug development”. AAPS J, 2025, Vol 27, art 142.
- Desai M et al, “Expert insights into the development of large-volume subcutaneous drugs with permeation enhancers: a survey examining challenges, alternatives, and future directions”. Int J Pharm, 2026, Vol 689, art 126515.

