To Issue 188
Citation: Johansson A, Rouf P, Hedge O, “PharmaShell – An ALD Nanocoating Technology for Once-Monthly Injectables”, ONdrugDelivery, Issue 188 (Jul 2026), pp 52–56.
Dr Anders Johansson, Dr Polla Rouf and Dr Oliver Hedge introduce Nanexa’s PharmaShell® technology and discuss how, in combination with nanotechnology, it can achieve previously unattainable dosing intervals with standard formulations.
Long-acting injectable therapies are transforming chronic disease management by reducing dosing frequency and improving patient adherence. PharmaShell® is a drug delivery technology designed to enable once-monthly injections for drugs that currently require frequent dosing. Developed by the Swedish company Nanexa, PharmaShell is centred on ultra-thin nanocoatings applied to drug microparticles using atomic layer deposition (ALD) – a precision technique adapted from the semiconductor industry.1
By encapsulating injectable drug particles in a nanometre-thick, biocompatible, inorganic coating, PharmaShell creates a controlled-release depot formulation. After injection, the coating dissolves at a tuned rate, providing a sustained therapeutic release over weeks to months.2 This approach enables high drug loading in a small-volume injection, eliminating the need for large implants or frequent dosing. In practice, formulations using PharmaShell can be delivered through thin needles (30G) with conventional syringes or autoinjectors, maximising patient comfort while ensuring prolonged drug action.
PHARMASHELL TECHNOLOGY & RATIONALE
The core principle of PharmaShell is to combine nanotechnology with pharmacotherapy to achieve dosing intervals unattainable with standard formulations. Particles of pure drug substance, typically in the range of a few microns, are enveloped with an extremely uniform PharmaShell coating (approximately 10–50 nm thick) using ALD. This atomic-level process provides unparalleled control over the coating thickness and composition, which, in turn, determines how quickly the drug is released once inside the body.
By adjusting parameters such as coating material (e.g. oxide type) and thickness, Nanexa can “dial in” a desired release profile; for example, this could be a near-linear release over 30 days or a slower three-month release for quarterly dosing. The impermeable coating initially protects the drug from immediate dissolution after injection, and then, as the coating gradually dissolves or becomes porous under physiological conditions, the drug is steadily released. This controlled dissolution mechanism contrasts with traditional poly(lactic-co-glycolic acid) (PLGA) microsphere depots, which often rely on polymer degradation, enabling formulators to avoid the high initial burst and unpredictable tail-off that can occur with those systems.3
The rationale for PharmaShell is clear: by flattening the pharmacokinetic curve and extending it, therapeutic drug levels can be maintained with one injection per month or potentially one injection every three months, instead of daily or weekly administration. This has major implications for patient convenience and compliance – fewer injections means reduced discomfort and increased adherence to treatment, particularly for chronic conditions such as diabetes, obesity or other diseases requiring long-term injectable therapies.
Furthermore, a more stable drug concentration (lower peak-to-trough variation) can translate to reduced side effects, as many adverse events are linked to peak plasma levels. Finally, reduced dosing frequency can potentially mitigate the effects of a missed dose, such as reducing the risk of therapeutic failure. PharmaShell’s ability to achieve stable, low-fluctuation drug levels over extended periods is therefore a key advantage in improving safety and tolerability.4
“PHARMASHELL COATINGS ARE INORGANIC AND DO NOT RELY ON ANY SPECIFIC DRUG-POLYMER CHEMISTRY, SO THE PLATFORM CAN BE APPLIED TO A WIDE RANGE OF MOLECULES – FROM SMALL-MOLECULE THERAPEUTICS TO LARGE PEPTIDES AND BIOLOGICS.”
Another key aspect of the technology is its broad applicability. PharmaShell coatings are inorganic and do not rely on any specific drug-polymer chemistry, so the platform can be applied to a wide range of molecules – from small-molecule therapeutics to large peptides and biologics. The coating process occurs at near ambient temperatures and has been shown to preserve the stability and activity of sensitive biomolecules, including peptides such as glucagon-like peptide-1 (GLP-1) analogues.
In addition, the inert nature of the ALD coating materials and their low mass fraction (often less than 10–20% of the total particle weight) means that they add minimal injection-site burden. The aluminium content in a PharmaShell dose (e.g. in a monthly semaglutide product) would be only a few hundred micrograms – far below the established safety thresholds for parenteral aluminium exposure5 and even less than typical dietary aluminium intake. This gives confidence that the coating materials serve their purpose as a delivery vehicle without introducing safety concerns.
ONCE-MONTHLY SEMAGLUTIDE DEPOT
Nanexa’s internal project on PharmaShell-coated semaglutide is a compelling example of PharmaShell’s potential in action. This project aims to develop a once-monthly depot formulation of semaglutide (a GLP-1 receptor agonist) for the treatment of type 2 diabetes and obesity. Semaglutide is currently marketed as Novo Nordisk’s Ozempic (for diabetes) and Wegovy (for obesity) in a once-weekly injection format – a significant improvement over daily injections, yet still requiring 52 injections per year. A monthly formulation would reduce this to just 12 injections per year, offering patients an even more convenient regimen while maintaining efficacy.6
The PharmaShell platform is particularly well-suited to semaglutide for several reasons. First, semaglutide is a relatively large peptide (~4 kDa), and the combination of its albumin-binding property and high bioavailability makes it a good candidate for extended release using PharmaShell. Second, its therapeutic mechanism (glucose control and appetite suppression) benefits from maintaining steady, basal levels rather than sharp peaks and troughs, which aligns perfectly with the profile delivered by a controlled-release depot.7 Finally, clinical use of semaglutide involves a dose-escalation phase (patients start at a low dose and gradually increase to mitigate side effects). A long-acting formulation can accommodate this by adjusting the initial dosing schedule (e.g. either administering a smaller PharmaShell-coated dose for the first one or two months before the full maintenance dose or a less frequent initial dosing regimen), which early simulations have shown to be feasible without compromising the smooth release profile.
Nanexa initiated development of PharmaShell-coated semaglutide in 2025, using knowledge from an earlier PharmaShell GLP-1 project. This earlier project provided a critical proof-of-concept in humans: a Phase I study using PharmaShell-coated liraglutide (in metformin-stable, GLP-1 naive, type 2 diabetic patients) demonstrated successful prolonged release and tolerability, with results presented at the American Diabetes Association Scientific Sessions in June 2025.8 In that first-in-human trial, a single injection of PharmaShell liraglutide achieved exposure over 36 days, effectively converting a daily injectable into a monthly dose.
This encouraging outcome laid the groundwork for switching to semaglutide, as the project with liraglutide strongly indicated that the PharmaShell approach could be translated into clinical practice. For semaglutide – a more potent and longer-acting molecule than liraglutide – the team anticipated that a once-monthly dose could potentially match or even surpass the clinical performance of weekly Ozempic/Wegovy.
“EARLY ON, NANEXA IDENTIFIED THAT MODIFICATION OF THE COATING COMPOSITION AND THICKNESS COULD DRAMATICALLY REDUCE THE INITIAL ‘BURST’ RELEASE THAT WAS OBSERVED WITH A PRIOR FORMULATION.”
RECENT PRECLINICAL RESULTS – ADVANCING A BETTER FORMULATION
The development has already yielded significant progress in Nanexa’s labs and preclinical studies. A key focus has been to optimise the PharmaShell coating and formulation specifically for semaglutide’s properties. Early on, Nanexa identified that modification of the coating composition and thickness could dramatically reduce the initial “burst” release that was observed with a prior formulation. In a comparative experiment, an optimised semaglutide-coated formulation showed a much flatter release profile in vivo than the earlier version used in the first liraglutide trial. Approximately 50% of the semaglutide dose was released over the first two weeks with the new formulation (roughly 25% per week), whereas the older formulation released ~50% of its payload in just the first week. This improvement means a more consistent drug level throughout the critical first month, and a lower peak concentration immediately post-dose.
In practical terms, the refined PharmaShell semaglutide achieves a near-linear release over at least one month, providing what is essentially a constant infusion profile from a single injection. Indeed, internally conducted rat pharmacokinetic studies (using a three-month model to assess long-term release) indicated that the plasma concentration of semaglutide can be maintained in a tight range for the full four- to five-week period with the new formulation. Notably, by minimising early release, the formulation is expected to reduce initial side effects, such as nausea and flushing, which are often dose- and Cmax-related for GLP-1 therapies.
Another significant finding comes from pharmacokinetic simulations and animal models regarding plasma concentration fluctuations. With monthly dosing, drug levels must not dip too low at end-of-interval or spike too high after each injection. Using data from preclinical studies, Nanexa simulated human plasma profiles for monthly semaglutide dosing.9 The results are highly promising: a peak-to-trough ratio of roughly 1.2 was predicted for steady-state monthly dosing and 1.5 for three-monthly dosing (depending on dose level). For context, a weekly semaglutide therapy itself has a peak-to-trough ratio of around 1.7–1.9 at steady state, as even with a weekly injection, levels rise and fall.
Thus, the PharmaShell monthly depot can achieve plasma level stability comparable with the current gold-standard weekly injection. Figure 1 illustrates this equivalence: the concentration-versus-time profile of the once-monthly PharmaShell semaglutide closely shadows that of once-weekly Wegovy (semaglutide), without extreme peaks or troughs. Simulations were made using an established model described by Overgaard et al.10 This flat profile is not only efficacious but also clinically important for safety – lower fluctuation means that the body is not subjected to high transient concentrations, likely translating to a lower incidence of side effects, such as the gastrointestinal events associated with GLP-1 agonists (data for Wegovy taken from publicly available information and overlaid on Nanexa’s data for comparison).6
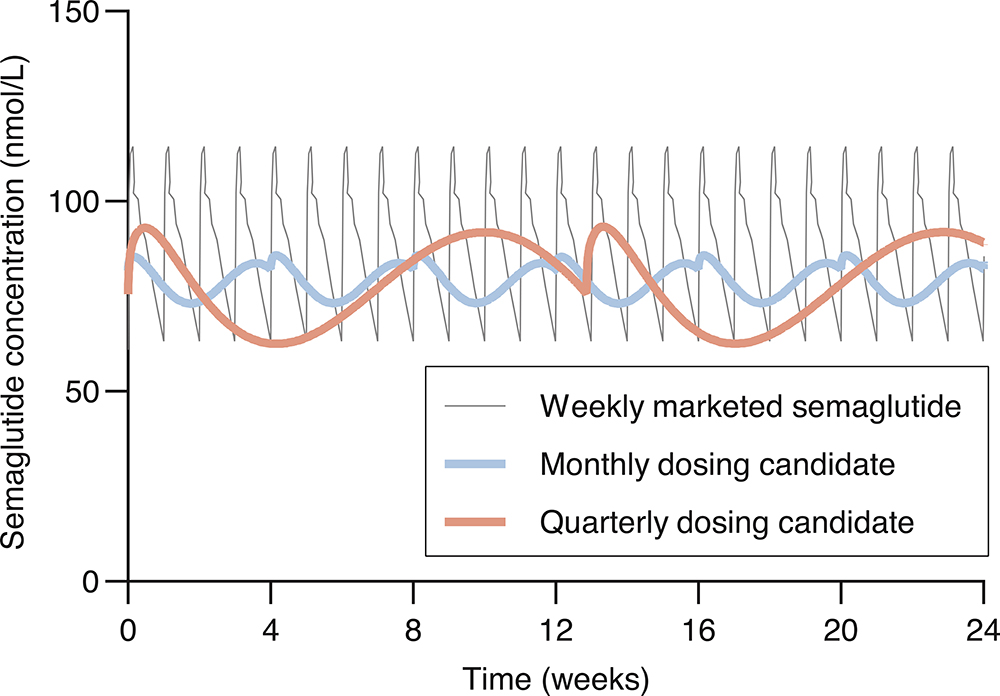
Figure 1: Predicted pharmacokinetic profiles for monthly PharmaShell semaglutide dosing, indicating a stable plasma concentration with lower peak-to-trough fluctuations comparable with weekly dosing of semaglutide (e.g. Wegovy).
Supporting these pharmacokinetic achievements, Nanexa has also addressed the formulation’s real-world usability. One significant advance in 2026 has been the development of a ready-to-use suspension formulation of PharmaShell-coated semaglutide particles. Earlier PharmaShell clinical trials used a two-vial system (dry coated powder reconstituted in a liquid at the time of injection). However, a single-vial or prefilled syringe system is far more convenient for the end user. By selecting a suitable non-aqueous vehicle and optimising the particle dispersion, Nanexa created a suspension that remains stable over time.
Ongoing stability studies have shown at least six months of real-time stability at room temperature and at 40°C for non-aqueous suspensions of PharmaShell-coated GLP-1 analogues, without any agglomeration of the particles or loss of performance or quality. Kinetic modelling indicates that a shelf life of 36 months at room temperature is feasible. In other words, the product can potentially be supplied in a prefilled syringe or cartridge, stored at ambient conditions and used directly by patients – a major practical advantage.
Additionally, the rheological properties of the suspension (e.g. viscosity) have been adjusted so that it can be administered through a fine-gauge needle. For an optimal patient experience, the use of a spring-powered autoinjector is envisioned – this would easily accommodate the slightly higher injection force and ensure a smooth administration even with a more viscous suspension. Other marketed long-acting injectables (e.g. AstraZeneca’s exenatide Bydureon® BCise™ autoinjector) have successfully implemented similar solutions, so the path for device combination is well established.
“NANEXA HAS BEGUN EXPLORATORY WORK
WITH DEVICE PARTNERS TO CONFIRM COMPATIBILITY OF THE PHARMASHELL SEMAGLUTIDE SUSPENSION WITH TYPICAL PREFILLED SYRINGES AND AUTOINJECTOR SYSTEMS, WITH NO ISSUES IDENTIFIED TO DATE.”
Nanexa has begun exploratory work with device partners to confirm compatibility of the PharmaShell semaglutide suspension with typical prefilled syringes and autoinjector systems, with no issues identified to date (e.g. no clogging, consistent dose delivery).
UPSCALE AND MANUFACTURING CONSIDERATIONS
As PharmaShell semaglutide advances toward clinical trials and commercialisation, a parallel effort is underway to scale up the PharmaShell manufacturing process. Unlike conventional drug formulation methods, ALD coating requires specialised equipment and process expertise. Nanexa is working to ensure that PharmaShell can transition from laboratory scale (grams of coated particles) to clinical and commercial scale (multi-kilogram batches) efficiently.
The coating process itself is modular and can be run in larger ALD reactors or in parallel across multiple reactor chambers. In fact, a dedicated scale-up installation for PharmaShell production is currently being explored. Plans include implementing a “1/10 scale” pilot ALD tool in Nanexa’s GMP facility in Uppsala as an intermediate step, which would demonstrate the ability to produce coated particles at one-tenth of the full commercial batch size. This pilot tool will inform the design and operation of a subsequent full-scale production ALD machine, capable of handling the quantities needed for global product supply. The ultimate goal is to have the PharmaShell semaglutide manufacturing process and equipment “launch-ready” in time for late-stage clinical trials and market introduction in the next few years.
Beyond the coating itself, other manufacturing aspects are also being scaled and optimised. Upstream, the drug particle engineering (micronisation or spray drying of semaglutide to the desired particle size) is conducted in partnership with CMOs experienced in pharmaceutical spray drying. Downstream, the fill-finish processes for the suspension are being adapted from existing practices used for depot injections. For instance, filling systems and appropriate container closure solutions are under evaluation to ensure that the final product can be filled, sterilised and packaged reliably. By proactively addressing scale-up challenges now, well ahead of product launch, Nanexa is de-risking the path to market.
SUMMARY
In summary, PharmaShell is an enabling technology that can reshape how injectable therapies are delivered. The example of PharmaShell semaglutide demonstrates how the platform can take a weekly biologic and convert it into a monthly treatment, with equal (or improved) therapeutic coverage and potentially fewer side effects. The technology’s recent preclinical successes – achieving linear month-long release and matching or outperforming the pharmacokinetics of the current standard of care – underline the viability of this approach.
Coupled with a clear strategy for manufacturing scale-up and device integration, commercially available PharmaShell-based products are moving steadily towards reality. If successful, they hold the promise of greatly simplifying treatment regimens for patients and unlocking new possibilities in chronic disease management. With its combination of nanotechnology precision and biomedical innovation, PharmaShell exemplifies the next generation of drug delivery systems, where one injection per month could soon replace a dozen injections or more – improving patients’ lives through smarter technology.
REFERENCES
- Kessels E et al, “Atomic layer deposition”. Nat Rev Methods Primers, 2025, Vol 5, art 66.
- Hellrup J et al, “Nanoshells prepared by atomic layer deposition – long acting depots of indomethacin”. Eur J Pharm Biopharm, 2019, Vol 140, pp 60–66.
- Butreddy A et al, “PLGA/PLA based long acting injectable depot microspheres in clinical use: production and characterization overview for protein/peptide delivery”. Int J Mol Sci, 2021, Vol 22(16), art 8884.
- “Product Quality Review: Exenatide extended release, non aqueous (BYDUREON BCISE)”. US FDA, 2017.
- “Draft Guidance for Industry: Small Volume Parenteral Drug Products and Pharmacy Bulk Packages for Parenteral Nutrition: Aluminum Content and Labeling Recommendations”. US FDA, Jul 2025.
- Yang XD, Yang YY, “Clinical pharmacokinetics of semaglutide: a systematic review”. Drug Des Devel Ther, 2024, Vol 18, pp 2555–2570.
- Gorgojo Martínez JJ et al, “Clinical recommendations to manage gastrointestinal adverse events in patients treated with GLP 1 receptor agonists: a multidisciplinary expert consensus”. J Clin Med, 2022, Vol 12(1), art 145.
- Devries H et al, “1975-LB: A Single Ascending Dose Study of a Once-Monthly Liraglutide Formulation in Participants with Type 2 Diabetes”. Diabetes, 2025, Vol 74(Suppl 1), art 1975-LB.
- Hellrup J, “PharmaShell®: Atomic layer deposition enabling once monthly and once quarterly semaglutide depots, with clinical proof of concept from liraglutide”. DDF Summit, 2026, Berlin, Germany.
- Overgaard RV et al, “Population Pharmacokinetics of Semaglutide for Type 2 Diabetes”. Diabetes Ther, 2019, Vol 10(2), pp 649–662.