Citation: Ecenarro Probst S, “The Capsule-Based DPI: An Environmentally Friendly & Efficient Dosage Form”. ONdrugDelivery Magazine, Issue 72 (Dec 2016), pp 8-11.
Susana Ecenarro Probst presents evidence, set against the backdrop of environmental concerns over HFC propellants in MDIs, supporting the adoption of dry-powder inhalers as an attractive alternative.
It has been a long and tough negotiation path since the international Montreal Protocol treaty was adopted on September 16, 1987. It was signed initially by 46 countries with the aim of regulating the production and use of chemicals, such as chlorofluorocarbons (CFCs) and halon, which were contributing to the depletion of the Earth’s ozone layer. On March 2, 1989, 12 European Community nations agreed to ban the production of all CFCs by the end of the century. The phasing-out commitment of these substances for the developing countries was extended to 2010.
CFCs had multiple applications in the field of refrigeration and air conditioning systems, heat pumps, insulation foams and pharmaceutical aerosols, among others. In the medical field, respiratory devices such as pressurised metered dose inhalers (pMDIs) had been manufactured with CFC propellants since their introduction in the sixties.
“HFCs have a warming effect of up to 3,800 times that of carbon dioxide,1 and these chemical substances are currently the world’s fastest growing greenhouse gases with an increase in emissions up to 10% each year.2 According to the UK NHS, the greenhouse effect of current UK emissions of HFCs from inhalers was in 2013 equivalent to 8% of the UK’s entire carbon footprint… ”
A new type of propellant for aerosols has since been developed, based on different technical and financial aspects, and accepted as a safer alternative to CFCs, the hydrofluorocarbon (HFC) group of chemical substances. The transition to this new propellant started in 1994 with the first non-CFC pMDI, Proventil HFA (salbutamol) which contained a hydrofluoroalkane (HFA), and continued through to the end of 2008 with some US FDA market withdrawals.
There has been much controversy in recent years around the fact that even though HFCs belong to the group of strong greenhouse gases, they were carefully selected as the best option to replace CFCs due to their lack of contribution to ozone layer depletion. Contrary to what might be assumed, HFCs have a warming effect of up to 3,800 times that of carbon dioxide,1 and these chemical substances are currently the world’s fastest growing greenhouse gases with an increase in emissions up to 10% each year.2 It is interesting to note that according to the UK NHS, in 2013 the greenhouse effect of current UK emissions of HFCs from inhalers was equivalent to 8% of the UK’s entire carbon footprint.3
A new investigational study co-authored by the researchers at the US National Oceanic and Atmospheric Administration (NOAA) Earth System Research Laboratory 4 shows that the contribution of HFCs to greenhouse warming could contribute to 10% of that of CO2 by 2050 if no specific measures are taken to restrict their use.
Recently, on October 15, 2016, the 28th Meeting of the Parties (MOP28), the most important climate conference since the Paris summit in 2015, gathered 197 Montreal Protocol members in Rigali, Rwanda (UNEP News). An agreement was adopted which implies challenging the compromise to initiate a HFCs phase-down by 2019 in developed countries, reaching an 85% reduction (based on 2011–2013 levels) by 2036. Due to financial restrictions and a High Ambient Temperature (HAT), some developing countries will be expected to adhere to a freeze on HFCs consumption levels starting in 2024 and other countries such as India in 2028.
“Contrary to what it is often believed, adults with severe respiratory diseases (severe asthma or COPD or acute exacerbations) can achieve “clinically relevant” PIFR through DPIs…”
However, the existing agreements could represent a limited impact since projections indicate a significant growth in the demand for HFCs in Asia, the Middle East, Latin America and Africa due to a fast-expanding middle class in some of these countries over the next decades.
According to current global environmental concerns, respiratory inhalers are already considered to represent a sizeable contribution to planet warming because of the propellant gases used in metered dose inhalers. They are, for example, some of the most commonly prescribed medications in the UK.5 Thus it is essential to ensure that inhaled drugs are recommended appropriately and used correctly to avoid unnecessary waste.
Dry powder inhalers (DPIs) have proven to be a very good alternative to pMDIs. They do not require propellants and have a carbon footprint 18 times lower than pMDIs, demonstrating that DPIs are a cleaner technology. Additionally, they are considered to be equally effective for the treatment of the most common respiratory diseases, asthma and COPD.6-7
Drug deposition in the lungs from capsule-based DPIs has been under scrutiny in several studies over the past few years (see “Respiratory Drug Delivery, Essential Theory and Practice”, Page 284, corresponding journal references included). The deposition value obtained from the Cyclohaler® (Teva, Petah Tikva, Israel). measured by gamma scintigraphy averaged 19% of the capsule dose and was similar in patients with mild or severe pulmonary impairment. However, some new particle engineering technology such as PulmoSphere® (Novartis, Basel Switzerland) particles achieved an in vivo average result of 34.3% by means of the Turbospin® device (PH&T, Milan, Italy). A different formulation using large porous particles with the AIR® inhaler (originally developed by Alkermes (Dublin, Ireland) produced a higher lung deposition average result of 51%.
In contrast, lung deposition from pMDIs produced values of around 20% and below, with a few results close to or above 40%. The higher figures came from a HFA solution formulation (QVAR®, Teva), which delivers an aerosol with a smaller mass median aerodynamic diameter than conventional pMDI suspension formulations.8 When analysing the factors that might influence the effectiveness of a capsule based DPI, the following characteristics should be taken into consideration:
1. Capsule-Based DPIs are Breath-Actuated Devices
This is considered an advantage since there is no “press and breathe” action that requires co-ordination, as with many pMDIs (except for breath-actuated pMDIs). The main consequence of poor inhaler handling, such as actuating the pMDI too late, is a low or variable lung dose that in turn leads to variable lung deposition. However, with capsule-based DPIs, some patients may not possess the required manual dexterity to load capsules, especially elderly patients or children, who could be hindered if the patient has a severe airflow obstruction.
The importance of patients receiving adequate instruction on how to use an inhaler has been addressed and emphasised at several conferences in the last years, revealing the important role that health professionals play in supporting patients by offering to monitor peak inspiratory flow rate (PIFR) and by showing them training aids.9
2. The Aerosol Formation in DPIs Usually Depends on the Inhalation Effort of the Patient
There is clear evidence that the total lung deposition will increase with a higher inspiratory flow rate (IFR) due to better dispersion of the powder. However, the time at which PIFR is achieved during inhalation is also relevant and depends on the type of DPI used. It is important that the PIFR be reached as soon as possible, since the delivered dose and the powder de-agglomeration occur primarily in the early part of inhalation.10 Contrary to what it is often believed, adults with severe respiratory diseases (severe asthma or COPD or acute exacerbations) can achieve “clinically relevant” PIFR through DPIs.11
“Several investigations have shown that the capsule plays an important part in delivery from capsule-based DPIs, because not only does it participate as packaging of the formulation, but it also has a role in the aerosolisation of the powder and the dispersion of the micronised drug from the carrier after the patient has pierced the capsule and inhaled through the DPI..”
The circumstance of suboptimal inhalation could cause insufficient powder disaggregation followed by a low emitted dose due to some dry powder being retained in the capsule and/or device. Additionally, the humidity (e.g. the moisture content of the capsule containing the drug powder, drastic environmental condition or exhalation during inhalation technique) is another factor that together with the inspiratory flow rate might affect the aerodynamic performance of a dry powder formulation.
Both parameters have been studied in an investigation carried out at the Laboratory of Pharmaceutics and Biopharmaceutics, Université Libre de Bruxelles (ULB, Belgium), by testing different inspiratory flow rates and by comparing the behaviour of gelatin and hypromellose (HPMC) capsules in drastic temperature and relative humidity conditions.12 The aim of this study was an aerodynamic performance assessment of a conventional formoterol based dry powder formulation (Formoterol content was 12 µg per 24 mg) using these conditions (Figure 1):
- Flow rates (30, 60 and 100 L/min)
- Storage conditions (4 h at 40°C 75% RH) to simulate patient misuse (e.g. exhalation) or inappropriate storage in a warm humid environment.

Figure 1: Experimental methods to evaluate the aerodynamic performance of a conventional formoterol-based dry powder formulation using two types of capsules (hypromellose & gelatin) from two manufacturers (Qualicaps® & Capsugel®).
Several investigations have shown that the capsule plays an important part in delivery from capsule-based DPIs, because not only does it participate as packaging of the formulation, but it also has a role in the aerosolisation of the powder and the dispersion of the micronised drug from the carrier after the patient has pierced the capsule and inhaled through the DPI.13
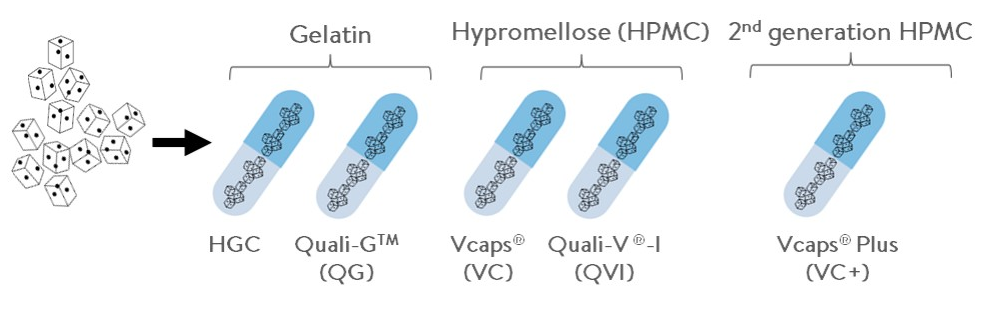
The two hard capsule types currently available in the pharma market are firstly the gelatin capsule, used as the pharmaceutical standard for more than 100 years, and secondly the HPMC capsule that has risen to the fore in recent years. HPMC has increased in popularity following a significant amount of pharmaceutical research showing that gelatin capsules are not suitable for encapsulating hygroscopic products, and are chemically unstable under certain conditions. HPMC capsules have emerged in the market as the most viable alternative because of their vegetal origin, chemical stability, absence of crosslinking and low moisture content (4.5-6.5%).
Within the framework of this study, the drug retention in the different types of capsule – Quali-V®-I manufactured by Qualicaps®, and Vcaps® / Vcaps® Plus manufactured by Capsugel® (Morristown, NJ, US) – was evaluated together with the fine particle dose (FPD ≤5 μm) expected to deposit in the peripheral part of the lungs (see Figure 1). A low resistance device, Axahaler® (SMB, Brussels, Belgium) was used connected to a Next Generation Impactor (NGI; Copley Scientific, Nottingham, UK).
The main conclusions of the investigation can be summarised as follows:
- At the optimal flow rate (100 L/min) the FPD was higher for HPMC capsules (Quali-V®-I and Vcaps®) in relation to gelatin capsules and the 2nd generation HPMC capsules (Vcaps® Plus).
- At the different flow rates corresponding to 30, 60 and 100 L/min, only the HPMC capsules (Quali-V®-I and Vcaps®) presented no differences in the FPD between 60 and 100 L/min. Therefore, more robust performances were observed with HPMC versus gelatin capsules that could be explained by the higher moisture content inherent in gelatin capsules (13-16% versus 4.5-6.5% for gelatin and HPMC capsules, respectively).
- The drug retention in the capsules at 100 L/min was lower in HPMC capsules (Quali-V®-I and Vcaps®) than in gelatin capsules and the 2nd generation HPMC capsules (Vcaps® Plus). Additionally, Quali-V®-I showed the lowest formoterol retention in the capsule at the different flow rates.
It is well known that the patient can generate different flow rates through his/her inhalation device relating to its resistance. The differences in device resistance could result in various clinically relevant PIFR. Therefore, an alternative delivery device should be taken into consideration if patients have a pulmonary impairment and are unable to generate the optimum pressure drop or peak IFR.
Additionally, it is important that the combination of the dry powder for inhalation and its capsules present high FPD with low dependency on a flow rate (between 60 and 100 L/min) and low capsule retention. HPMC capsules showed higher and more robust FPD at this flow rate range than gelatin capsules, in particular Quali-V®-I with the lowest capsule retention at all tested flow rates. However, it is very important to avoid exposing the capsules to adverse conditions, which could affect significantly the aerodynamic performance of dry powder, regardless of the kind of capsules used.
CONCLUSION
The delivery of respiratory drugs via capsule-based DPIs offers an environmentally friendly alternative, as these devices enable the possibility of reducing a major source of greenhouse emissions over the years. The gradual transition is aligned as well with the new Rigali climate summit measures decided and agreed recently this year by almost 200 countries worldwide.
As presented in this article, both types of inhalation delivery system – capsule-based DPIs and pMDIs – are considered to be equally effective, so an expected acceptable clinical outcome for patients is ensured.
On the other hand, capsule-based DPIs are breath-actuated devices and avoid the often low and variable lung dose resulting from poor pMDI handling techniques.
The capsule behaves as the primary packaging material for the drug formulation and is considered an important part of the inhalation system because it participates in the aerosolisation of the powder and the dispersion of the micronized drug from the carrier after piercing the capsule. HPMC capsules have been shown to produce improved results compared with gelatin capsules with regard to the FPD and drug powder retention in the capsule.
Finally, the general ecological and sound scientific approach of capsule-based DPIs is in line with patient preferences. Nevertheless, it is in the hands of clinicians and policy makers to implement the adequate changes and to properly inform patients in order to consider switching to this more sustainable option.
REFERENCES
- Okamura S, Ashford P, Jackson J, Watterson J, “HFC consumption and emissions forecasting”. Report to UK Department for Environment, Food & Rural Affairs (prepared by AEA Technology PLC), 2011.
- United Nations Environmental Program (UNEP) News Centre.
- Hillman T, Mortimer F, Hopkinson N, “Inhaled drugs and global warming: time to shift to dry powder inhalers”. BMJ, 2013, Vol 346, f3359.
- Velders et al, “Future atmospheric abundances and climate forcings from scenarios of global and regional hydrofluorocarbon (HFC) emissions”. Atmospheric Environment, 2015, Vol 122, pp 200-209.
- UK National Institute for Health and Clinical Excellence (NICE) Clinical Guideline, “Chronic Obstructive Pulmonary Disease. Costing report— implementing NICE guidance”. February 2011.
- Dolovich MB, Ahrens RC, Hess DR, Anderson P, Dhand R, Rau JL, et al, “Device selection and outcomes of aerosol therapy: evidence-based guidelines”. Chest, 2005, Vol 127, pp 335-371.
- Shepherd J, Rogers G, Anderson R, Main C, Thompson-Coon J, Hartwell D, et al, “Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in adults and children aged 12 years and over”. Health Technol Assess, 2008, Vol12(iii-iv), pp 1- 360.
- Borgström et al, “Degree of throat deposition can explain the variability in lung deposition of inhaled drugs”. J Aerosol Med, 2006, Vol 19, pp 473-483.
- Al-Showair et al, “Can all patients with COPD use the correct inhalation flow with all inhalers and does training help?”Respir Med, 2007, Vol 101, pp 2395-2401.
- Chavan V, Dalby R, “Effect on rise in simulated inspiratory flow rate and carrier particle size on powder emptying from dry powder inhalers”. AAPS Pharm Sci, 2000, Vol 2, E10 [Abstract].
- Borgström L, “On the use of dry powder inhalers in situations perceived as constrained”. J Aerosol Med, 2001, Vol 14, pp 281-287.
- Wauthoz N, “Influence of Flow Rate and Usage in Drastic Condition on the Aerodynamic Performance of a Formoterol Dry Powder Formulation using different kinds of capsule”. Abstract at AAPS Annual Meeting, 2016 (Denver, CO, US).
- Coates MS, Fletcher DF, Chan HK, Paper JA, “The role of capsule on the performance of a dry powder inhaler using computational and experimental analyses”. Pharm Res, 2005, Vol 22(6), pp 923-932.