To Issue 187
Citation: Babaee S, “Oral Delivery of Macromolecules: Challenges and Opportunities for Device-Enabled GI Delivery”, ONdrugDelivery, Issue 187 (Jun 2026), pp 10–13.
Dr Sahab Babaee discusses the potential of device-based approaches to enable the delivery of macromolecules via the gastrointestinal tract, considering the constraints and possibilities of mucosal delivery devices, as well as the technologies currently being investigated to make this potential a reality.
Macromolecules, including biologics such as peptides, proteins and nucleic acids, are large, complex molecules that represent a major segment of the pharmaceutical market. Over the last several years, there has been growth in biologics license applications (BLAs) and approvals (Figure 1), with a market valuation around US$450 billion (£335 billion) in 2025 and projected to more than double to over $1 trillion by 2035, growing at a compound annual growth rate of about 8–10%.1–3
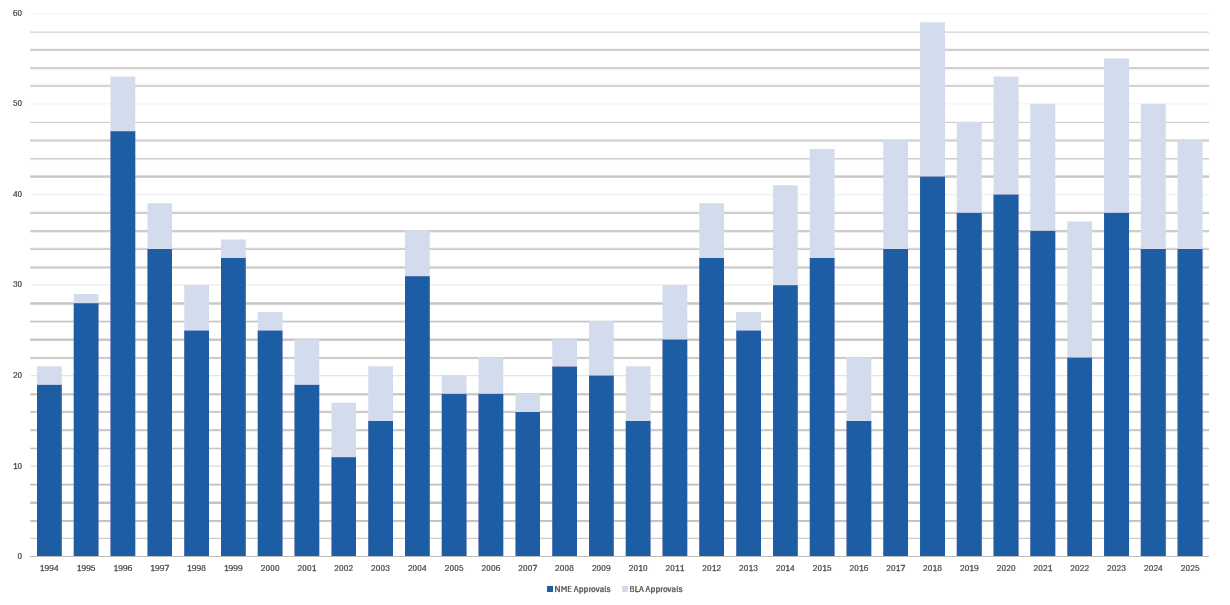
Figure 1: Paradigm shift from small molecules to biologics. Annual numbers of new molecular entities (NMEs) and BLAs approved by the US FDA’s Center for Drug Evaluation and Research since 1994.3
This growth is driven by rising demand across major therapeutic areas, including oncology, immunology, rare diseases and haematology, along with continued expansion into infectious disease, metabolic and cardiovascular indications. Currently, biologics are primarily administered via subcutaneous or intravenous routes, which present barriers to compliance, patient preference and accessibility. Oral gastrointestinal (GI) delivery represents a viable alternative to improve patient convenience and potentially reduce treatment burden.
KEY CHALLENGES IN ORAL DELIVERY OF MACROMOLECULES
The main barriers to oral delivery of biologics, which contribute to their poor efficacy, are:
- Poor Stability: Biologics exhibit poor stability due to their complex structures and large molecular sizes
- Rapid Degradation: Large molecules undergo rapid degradation when exposed to gastric acid and GI enzymes, making them inactive
- Poor Absorption: Absorption is limited due to the poor permeability of biologic drugs across the GI epithelium (i.e. inability to effectively cross mucosal barriers and overcome first‑pass metabolism)
- Low Bioavailability: Due to rapid degradation and poor absorption, orally administered biologics typically have very low bioavailability – often less than 2%.
“TO ADDRESS THESE CHALLENGES, DEVICE‑BASED STRATEGIES HAVE BEEN DEVELOPED TO BYPASS EPITHELIAL BARRIERS AND INJECT DRUGS DIRECTLY INTO THE GI SUBMUCOSA, REFERRED TO AS ORAL LOCAL MUCOSAL DELIVERY.”
To address these challenges, device‑based strategies have been developed to bypass epithelial barriers and inject drugs directly into the GI submucosa, referred to as oral local mucosal delivery. This approach results in significantly higher bioavailability compared with conventional non‑mucosal oral delivery, such as oral suspensions, and can achieve bioavailability comparable with or exceeding subcutaneous injection. Mucosal targeting GI delivery also offers a range of advantages over parenteral routes, which include:
- Non-invasive, painless delivery without the use of needles
- The ability for self‑administration and improved patient convenience
- Higher rates of patient adherence
- Increased bioavailability through enhanced local and/or systemic drug exposure.
In addition, mucosal delivery enables the administration of macromolecules or highly sensitive pharmacologic agents that are challenging to deliver via a non‑mucosal oral route and mitigates first‑pass hepatic metabolism.4
DESIGN REQUIREMENTS FOR GI MUCOSAL DELIVERY
Oral Delivery and Transit
The device needs to have an appropriate size and morphology to allow safe ingestion (e.g. a standard size 00 ingestible capsule) and passage through narrow orifices of the GI tract, such as the oesophagus, to reach the intended target site (e.g. stomach or intestines) without the need for endoscopy. Common design approaches include shape-shifting mesoscale devices and micro-architectures embedded within capsule platforms via non-endoscopic delivery.
Deployment and Positioning
The device must be capable of adopting the correct configuration, position and orientation at the target site to perform its intended function. Deployment may be self-actuated or triggered by internal or external stimuli. Considerations include whether deployment is targeted or random, and whether positioning is independent or dependent on local anatomy or physiological forces.
Activation and Drug Delivery
The device must reliably perform its intended therapeutic or diagnostic function. Functional modalities may include therapeutic interventions (e.g. drug delivery), diagnostic capabilities (e.g. sensing, monitoring, gripping, wireless communication, etc) or combined functions. Devices may operate as sensors and/or actuators and may be passive or active (i.e. pre-programmed or capable of real-time interaction). Long-term retention within the GI tract is generally challenging and often undesirable due to the risk of obstruction, particularly at the pylorus, except for small-molecule therapies.
Safe Removal and Exit
The device must ensure safe passage through the GI tract and, ultimately, exit the body without risk of obstruction or perforation. Removal strategies may include dissociable or biodegradable designs, as well as “ingest and recover” approaches, in which the ingestible device is naturally excreted and retrieved from stool (e.g. capsule endoscopy). Manual removal via endoscopic retrieval by a GI specialist is generally undesirable.
Safety Considerations
Safety plays a key role in the design and development of GI technologies, with two primary factors governing the safety of ingestible devices in the GI tract. First, device size and shape must allow safe passage through the narrow anatomical regions of the GI tract without presenting sharp features. Devices exceeding critical size thresholds (typically > 3 cm) pose an obstruction risk and may require surgical removal. Current constraints on electronics and battery miniaturisation can limit size reduction and increase this risk. Second, depth of penetration and interaction with the GI wall must be carefully controlled to avoid perforation, injury or bleeding. The gastric cavity provides a greater safety margin due to its thicker wall (about 4–8 mm) compared with the intestine (about 0.5–2 mm), resulting in more restrictive allowable penetration depths in intestinal applications.5–7
“VARIOUS DEVICE-BASED TECHNOLOGIES HAVE BEEN DEVELOPED AND INVESTIGATED TO OVERCOME THE EPITHELIAL CELL LAYER OF THE GI TRACT IN ORDER TO DELIVER THERAPEUTIC PAYLOADS TO THE GI SUBMUCOSA.”
GI DEVICE DEVELOPMENT: PHYSICAL MODES OF DELIVERY
GI drug-device combination technologies have been adapted from principles originally developed for transdermal drug delivery systems.7 Various device-based technologies have been developed and investigated to overcome the epithelial cell layer of the GI tract to deliver therapeutic payloads to the GI submucosa. These devices use physical modes of drug delivery that include, but are not limited to:6–8
- Needle-Free (Jet) Injection: A high-pressure fluid jet penetrates the GI mucosa to deliver macromolecules through a nozzle orifice, achieving robust bioavailability and immune responses. This approach represents the leading device-based strategy for oral GI drug delivery devices.9–11
- Needle-Based Injection: Ingestible capsules deploy a solid or soluble needle to inject macromolecules into GI tissue without requiring endoscopy.12
- Iontophoresis: An electrically assisted delivery method that enhances transport of charged therapeutics or macromolecules across GI epithelial barriers using low‑intensity electric currents.13
- Low-Frequency and Focused Ultrasound: Acoustic energy is used to transiently enhance GI epithelial permeability and local transport via induced oscillation or collapse of microbubble cavitation, enabling rapid and targeted delivery of large molecules.14,15
- Thermally Triggered Delivery: Heat-assisted delivery strategies are employed to modulate drug release or act as absorption enhancers by increasing mucosal transport and epithelial permeability, such as thermo-responsive hydrogels.16
- Magnetic: External magnetic fields have been explored as a means of enhancing the targeting of macromolecules within the GI tract via the use of magnetically responsive nanoparticles.17,18
SUMMARY & OUTLOOK
Despite advances in the development of new GI technologies over recent years, oral mucosal delivery of macromolecules via the GI tract remains challenging due to several key constraints, including the rapid degradation and poor absorption of large molecules, as well as technical and safety challenges associated with the design of ingestible devices. This article has reviewed device-driven strategies, which employ a device to physically perturb the GI epithelium and deposit drug depots directly into the submucosa. Many of these technologies are currently being explored in preclinical or early clinical studies and have demonstrated promising results. However, except for a limited number of devices, their safety and efficacy have yet to be fully established in late‑stage clinical trials.
“THIS FIELD REPRESENTS A PROMISING YET CHALLENGING TARGET SPACE FOR INNOVATION AND A KEY OPPORTUNITY FOR CONTINUED INVESTMENT, WITH THE POTENTIAL TO DELIVER SUBSTANTIAL THERAPEUTIC BENEFITS TO PATIENTS AND SIGNIFICANT VALUE TO THE BIOPHARMACEUTICAL SECTOR.”
As such, this field represents a promising yet challenging target space for innovation and a key opportunity for continued investment, with the potential to deliver substantial therapeutic benefits to patients and significant value to the biopharmaceutical sector. It is also worth noting that non-device-based strategies aimed at enhancing the stability and/or absorption of oral GI biologics are also attracting increasing interest and advancing rapidly in parallel with drug-device combination approaches, paving the way for the development of novel GI-based drug delivery platforms.
REFERENCES
- “Biologics Market Size, Scope, Revenue Report 2026 to 2035”. Market Report, InsightAce Analytic, Feb 2026.
- Langer R, “Delivery of macromolecular drugs: An update”. Q Rev Biophys, 2025, Vol 58, art e19.
- Mullard A, “2025 FDA approvals”. Nat Rev Drug Discov, 2026, Vol 25(2), pp 81–87.
- Homayun B, Lin X, Choi H-J, “Challenges and Recent Progress in Oral Drug Delivery Systems for Biopharmaceuticals”. Pharmaceutics, 2019, Vol 11(3), art 129.
- Abramson A et al, “An ingestible self-orienting system for oral delivery of macromolecules”. Science, 2019, Vol 363(6427), pp 611–615.
- Chu JN, Traverso G, “Foundations of gastrointestinal-based drug delivery and future developments”. Nat Rev Gastroenterol Hepatol, 2022, Vol 19(4), pp 219–238.
- Byrne J et al, “Devices for drug delivery in the gastrointestinal tract: A review of systems physically interacting with the mucosa for enhanced delivery”. Adv Drug Deliv Rev, 2021, Vol 177, art 113926.
- Caffarel-Salvador E et al, “Oral delivery of biologics using drug-device combinations”. Curr Opin Pharmacol, 2017, Vol 36, pp 8–13.
- Mitragotri S, “Current status and future prospects of needle-free liquid jet injectors”. Nat Rev Drug Discov, 2006, Vol 5(7), pp 543–548.
- Aran K et al, “An oral microjet vaccination system elicits antibody production in rabbits”. Sci Transl Med, 2017, Vol 9(380), art eaaf6413.
- Arrick G et al, “Cephalopod-inspired jetting devices for gastrointestinal drug delivery”. Nature, 2024, Vol 636(8042), pp 481–487.
- Abramson A et al, “Oral delivery of systemic monoclonal antibodies, peptides and small molecules using gastric auto-injectors”. Nat Biotechnol, 2022, Vol 40(1), pp 103–109.
- Byrne J et al, “Local iontophoretic administration of cytotoxic therapies to solid tumors”. Sci Transl Med, 2015, Vol 7(273), art 273ra14.
- Schoellhammer CM et al, “Ultrasound-mediated gastrointestinal drug delivery”. Sci Transl Med, 2015, Vol 7(310), art 310ra168.
- Schoellhammer CM, Langer R, Traverso G, “Of microneedles and ultrasound: Physical modes of gastrointestinal macromolecule delivery”. Tissue Barriers, 2016, Vol 4(2), art e1150235.
- Szunerits S, Boukherroub R, “Heat: A Highly Efficient Skin Enhancer for Transdermal Drug Delivery”. Front Bioeng Biotechnol, 2018, Vol 6, art 15.
- Price PM et al, “Magnetic Drug Delivery: Where the Field Is Going”. Front Chem, 2018, Vol 6, art 619.
- Chen W et al, “A magnetically actuated robotic capsule endoscope for in-situ visualization and microneedle-mediated targeted drug delivery in gastrointestinal tract”. Microsyst Nanoeng, 2026, Vol 12(1), art 42.